

Postoperative Outcomes Analysis After Pancreatic Duct Occlusion: A Safe Option to Treat the Pancreatic Stump After Pancreaticoduodenectomy in Low-Volume Centers
- PMID: 34993230
- PMCID: PMC8725883
- DOI: 10.3389/fsurg.2021.804675
Postoperative Outcomes Analysis After Pancreatic Duct Occlusion: A Safe Option to Treat the Pancreatic Stump After Pancreaticoduodenectomy in Low-Volume Centers
Abstract
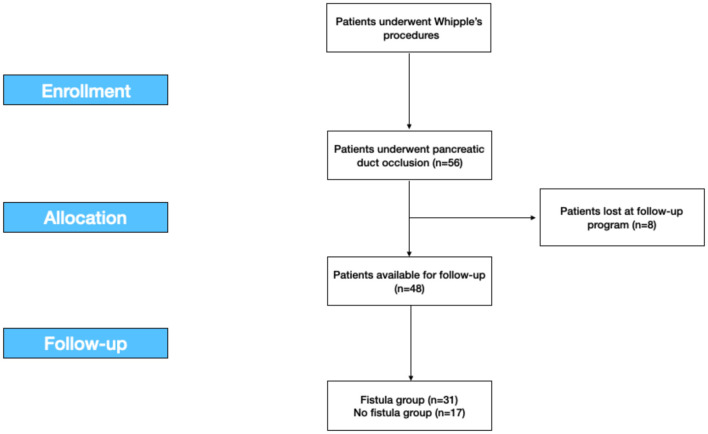
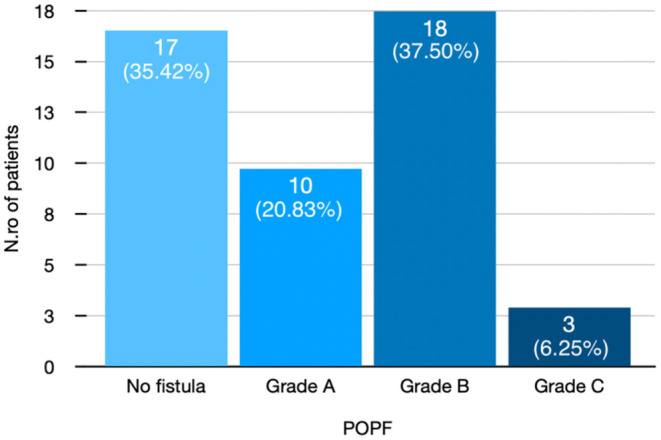
Background: Surgical resection is the only possible choice of treatment in several pancreatic disorders that included periampullar neoplasms. The development of a postoperative pancreatic fistula (POPF) is the main complication. Despite three different surgical strategies that have been proposed-pancreatojejunostomy (PJ), pancreatogastrostomy (PG), and pancreatic duct occlusion (DO)-none of them has been clearly validated to be superior. The aim of this study was to analyse the postoperative outcomes after DO. Methods: We retrospectively reviewed 56 consecutive patients who underwent Whipple's procedure from January 2007 to December 2014 in a tertiary Hepatobiliary Surgery and Liver Transplant Unit. After pancreatic resection in open surgery, we performed DO of the Wirsung duct with Cyanoacrylate glue independently from the stump characteristics. The mean follow-up was 24.5 months. Results: In total, 29 (60.4%) were men and 19 were (39.6%) women with a mean age of 62.79 (SD ± 10.02) years. Surgical indications were in 95% of cases malignant diseases. The incidence of POPF after DO was 31 (64.5%): 10 (20.8%) patients had a Grade A fistula, 18 (37.5%) Grade B fistula, and 3 (6.2%) Grade C fistula. No statistical differences were demonstrated in the development of POPF according to pancreatic duct diameter groups (p = 0.2145). Nevertheless, the POPF rate was significantly higher in the soft pancreatic group (p = 0.0164). The mean operative time was 358.12 min (SD ± 77.03, range: 221-480 min). Hospital stay was significantly longer in patients who developed POPF (p < 0.001). According to the Clavien-Dindo (CD) classification, seven of 48 (14.58%) patients were classified as CD III-IV. At the last follow-up, 27 of the 31 (87%) patients were alive. Conclusions: Duct occlusion could be proposed as a safe alternative to pancreatic anastomosis especially in low-/medium-volume centers in selected cases at higher risk of clinically relevant POPF.
Keywords: COVID-19 pandemic; POPF; duct occlusion; low-volume center; pancreatic cancer; pancreatic stump; pancreatic surgery.
Copyright © 2021 Giuliani, Avella, Segreto, Izzo, Buondonno, Coluzzi, Cappuccio, Brunese, Vaschetti, Scacchi, Guerra, Amato, Calise and Rocca.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources