

Cardiac magnetic resonance in the assessment of pericardial abnormalities: a case series
- PMID: 34993400
- PMCID: PMC8728722
- DOI: 10.1093/ehjcr/ytab444
Cardiac magnetic resonance in the assessment of pericardial abnormalities: a case series
Abstract
Background: Cardiac magnetic resonance (CMR) has a unique role in evaluating pericardial disease, permitting non-invasive tissue analysis, and haemodynamic assessment.
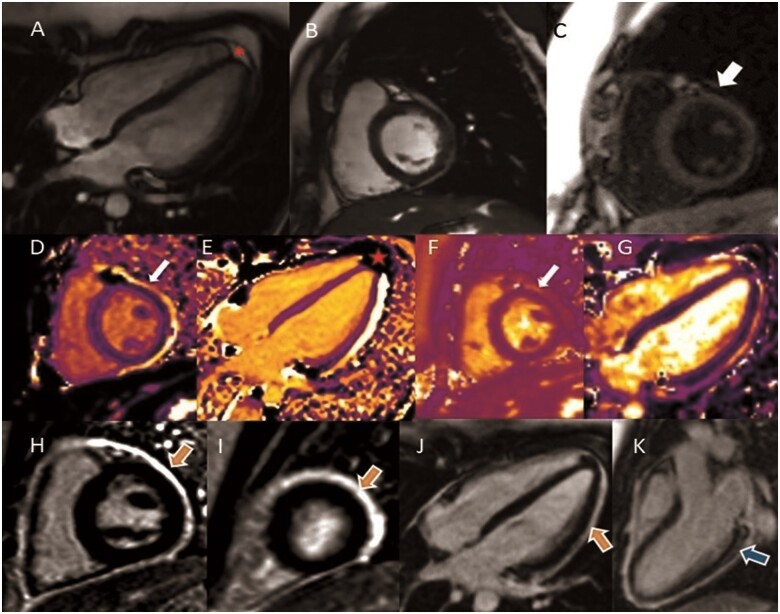
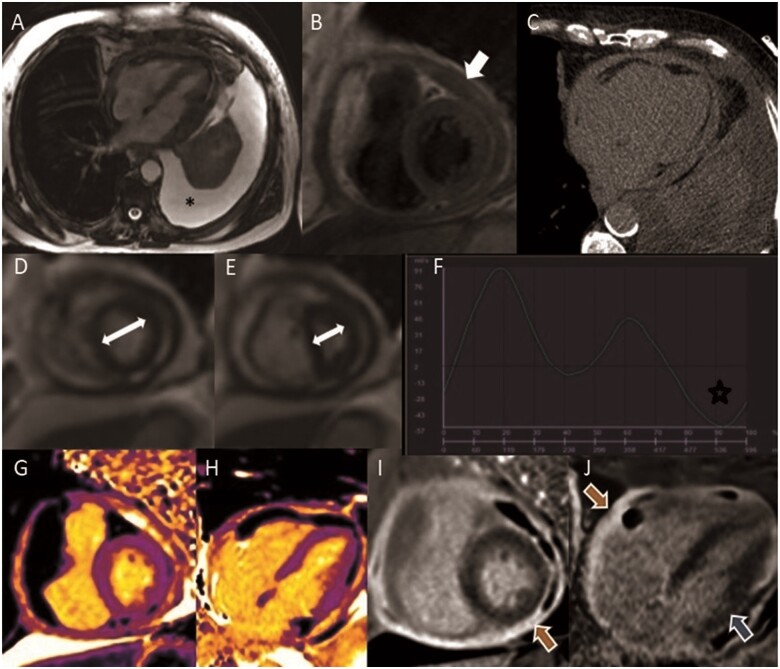
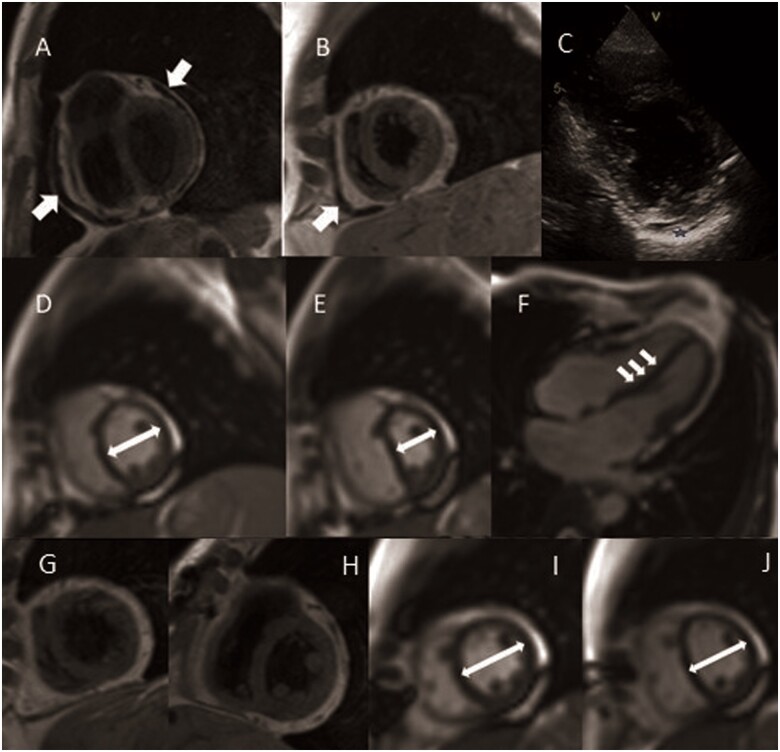
Case summary: In Case 1 of recurrent pericarditis, CMR confirmed reactivation of inflammation with late gadolinium enhancement and native T1/T2 mapping techniques, prompting therapeutic changes. In constrictive pericarditis, CMR is the only modality capable of differentiating a subacute potentially reversible form (Case 2), from a chronic, burnt out irreversible phase characterized by constrictive physiology (Case 3).
Discussion: Cardiac magnetic resonance is an effective tool to tailor individual therapy, particularly in cases of recurrent and constrictive pericarditis. Late gadolinium enhancement provides diagnostic and prognostic information, and multiparametric mapping has emerged as a promising tool with incremental diagnostic value.
Keywords: Cardiac magnetic resonance; Case series; Constrictive pericarditis; Pericardial disease; Pericarditis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

References
-
- Chetrit M, Xu B, Kwon D, Ramchand J, Rodriguez RE, Tan CD. et al. Imaging-guided therapies for pericardial diseases. JACC Cardiovasc Imaging 2020;13:1422–1437. - PubMed
-
- Zurick A, Bolen M, Kwon D, Tan CD, Popovic ZB, Rajeswaran J. et al. Pericardial delayed hyperenhancement with CMR imaging in patients with constrictive pericarditis undergoing surgical pericardiectomy - a case series with histopathological correlation. J Am Coll 2011;4:1180–1191. - PubMed
-
- Vidalakis E, Kolentinis M, Gawor M, Vasquez M, Nagel E.. CMR in pericardial diseases - an update. Curr Cardiovasc Imaging Rep 2020;13:14.
-
- Cosyns B, Plein S, Nihoyanopoulos P, Smiseth O, Achenbach S, Andrade MJ, et al. ; European Society of Cardiology Working Group (ESC WG) on Myocardial and Pericardial diseases. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging 2015;16:12–31. - PubMed
-
- Hassan O, Kwon D.. Update on MRI techniques for evaluation of pericardial disease. Curr Cardiol Rep 2020;22:147. - PubMed
Publication types
LinkOut - more resources
Full Text Sources