

Symptom Presentation and Access to Medical Care in Patients With Postural Orthostatic Tachycardia Syndrome: Role of Sex
- PMID: 34993433
- PMCID: PMC8712580
- DOI: 10.1016/j.cjco.2021.08.014
Symptom Presentation and Access to Medical Care in Patients With Postural Orthostatic Tachycardia Syndrome: Role of Sex
Abstract
Background: Postural orthostatic tachycardia syndrome (POTS) is a chronic form of orthostatic intolerance that primarily impacts female patients of childbearing age. The role of sex differences in POTS is not well understood. We sought to identify sex differences in diagnosis, symptoms, comorbidities, and treatments in female and male patients diagnosed with POTS.
Methods: A comprehensive survey was designed in partnership by Dysautonomia International (East Moriches, NY) and Vanderbilt University Medical Center (Nashville, TN). Patients were recruited through Dysautonomia International's website and social media channels. The survey was delivered online through a secure research data capture database. Responses were analyzed according to biological sex. Continuous variables are presented as median (25th percentile-75th percentile), and categorical variables are presented as number and proportion of participants.
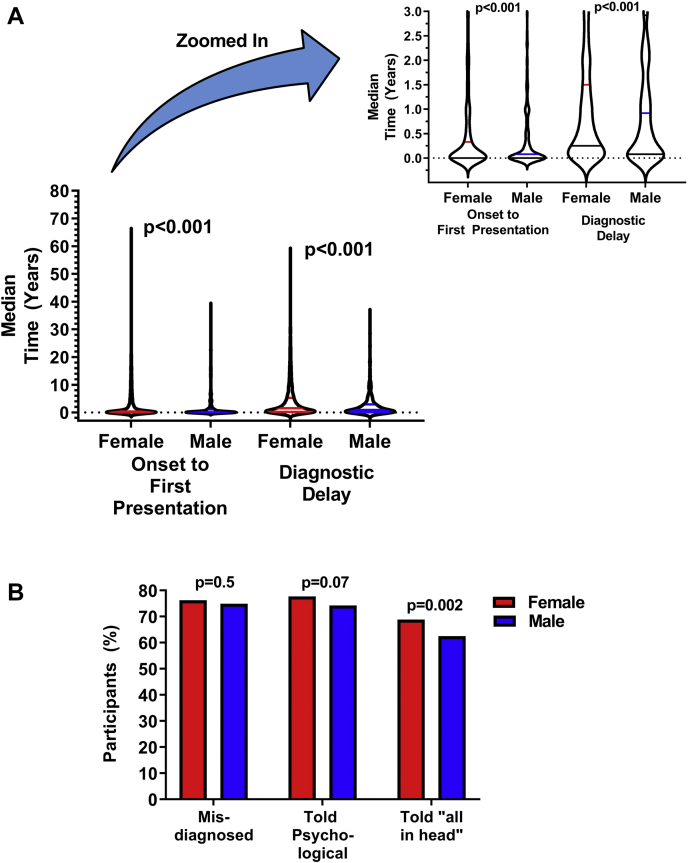
Results: A total of 8919 patients reported a physician diagnosis of POTS and were included in this analysis. The majority of respondents were female (93.7%). Female and male patients experienced misdiagnosis at similar rates (76.2% vs 74.9%, P = 0.5) and saw a similar number of doctors before diagnosis (5 [3-8] vs 5 [3-8], P = 0.9). Despite these similarities, diagnostic delay was longer for female, compared with male, patients (1.50 [0.25-5.25] years vs 0.92 [0.08-2.91] years, P < 0.001).
Conclusions: Despite the primarily female demographic of POTS patients, female patients experience more challenges with diagnosis than male patients. Increased awareness and recognition of POTS may help to reduce the diagnostic challenges in both female and male patients, and improve treatment and management for individuals living with this debilitating disorder.
Contexte: Le syndrome de tachycardie orthostatique posturale (STOP) est une forme chronique d’intolérance orthostatique qui touche principalement les femmes en âge de procréer. L’incidence du sexe sur le STOP n’est pas bien comprise. Nous avons cherché à déterminer les différences entre les sexes en ce qui a trait au diagnostic, aux symptômes, aux comorbidités et aux traitements chez les patients féminins et masculins ayant reçu un diagnostic de STOP.
Méthodologie: Une enquête exhaustive a été conçue en partenariat par Dysautonomia International (East Moriches, NY, États-Unis) et le Vanderbilt University Medical Center (Nashville, TN, États-Unis). Les patients ont été recrutés par l’entremise du site Web de Dysautonomia International et des médias sociaux. L’enquête a été réalisée en ligne au moyen d’une base de données sécurisée de saisie de données de recherche. Les réponses ont été analysées en fonction du sexe biologique. Les variables continues sont présentées sous forme de médiane (25e percentile-75e percentile), et les variables nominales sont présentées sous forme de nombre et de proportion de participants.
Résultats: Au total, 8 919 patients ont signalé un diagnostic de STOP établi par un médecin et ont été inclus dans cette analyse. La majorité des répondants étaient des femmes (93,7 %). Les patients de sexe féminin et masculin ont été mal diagnostiqués dans des proportions similaires (76,2 % vs 74,9 %, p = 0,5) et ont vu un nombre similaire de médecins avant le diagnostic (5 [3-8] vs 5 [3-8], p = 0,9). Malgré ces similitudes, le retard de diagnostic était plus long chez les femmes que chez les hommes (1,50 [0,25-5,25] an contre 0,92 [0,08-2,91] an, p < 0,001).
Conclusions: Même si les patients atteints de STOP sont principalement des femmes, ces dernières ont plus de difficultés à recevoir un diagnostic que les hommes. Une meilleure connaissance et reconnaissance du STOP peut contribuer à réduire les problèmes liés au diagnostic chez les patients féminins et masculins, et à améliorer le traitement et la prise en charge des personnes atteintes de ce trouble débilitant.
© 2021 The Authors.
Figures
References
-
- Thieben M.J., Sandroni P., Sletten D.M., et al. Postural orthostatic tachycardia syndrome: the Mayo clinic experience. Mayo Clin Proc. 2007;82:308–313. - PubMed
-
- Raj S.R., Guzman J.C., Harvey P., et al. Canadian Cardiovascular Society position statement on postural orthostatic tachycardia syndrome (POTS) and related disorders of chronic orthostatic intolerance. Can J Cardiol. 2020;36:357–372. - PubMed
-
- Benrud-Larson L.M., Dewar M.S., Sandroni P., et al. Quality of life in patients with postural tachycardia syndrome. Mayo Clin Proc. 2002;77:531–537. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
