

Management Trends and Outcomes of Patients Undergoing Radical Cystectomy for Urothelial Carcinoma of the Bladder: Evolution of the University of Southern California Experience over 3,347 Cases
- PMID: 34994657
- PMCID: PMC8746892
- DOI: 10.1097/JU.0000000000002242
Management Trends and Outcomes of Patients Undergoing Radical Cystectomy for Urothelial Carcinoma of the Bladder: Evolution of the University of Southern California Experience over 3,347 Cases
Abstract
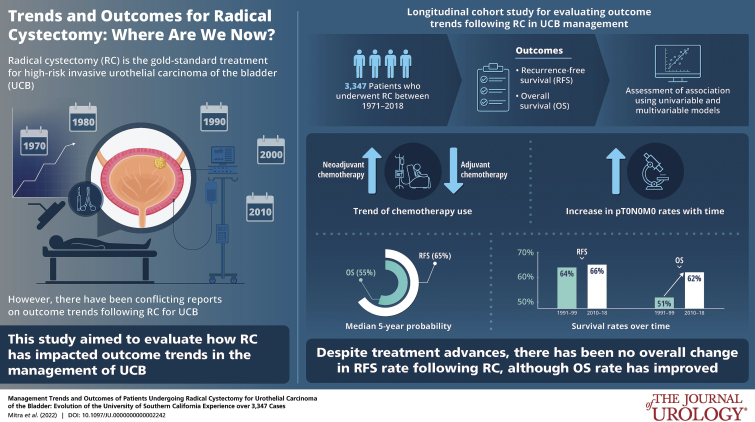
Purpose: There are conflicting reports on outcome trends following radical cystectomy (RC) for bladder cancer.
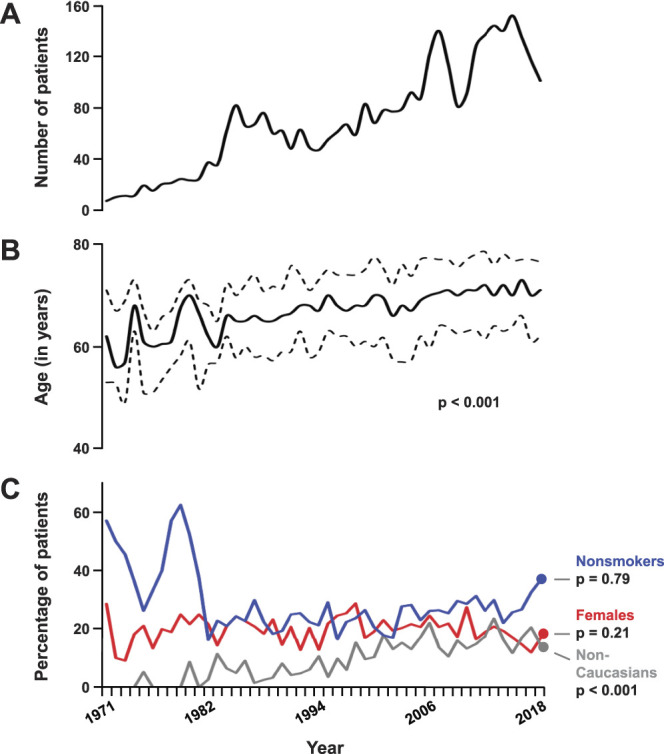
Materials and methods: Evolution of modern bladder cancer management and its impact on outcomes was analyzed using a longitudinal cohort of 3,347 patients who underwent RC at an academic center between 1971 and 2018. Outcomes included recurrence-free survival (RFS) and overall survival (OS). Associations were assessed using univariable and multivariable models.
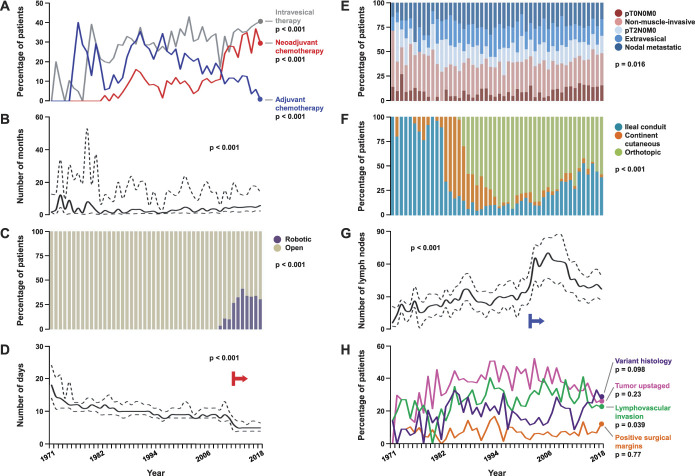
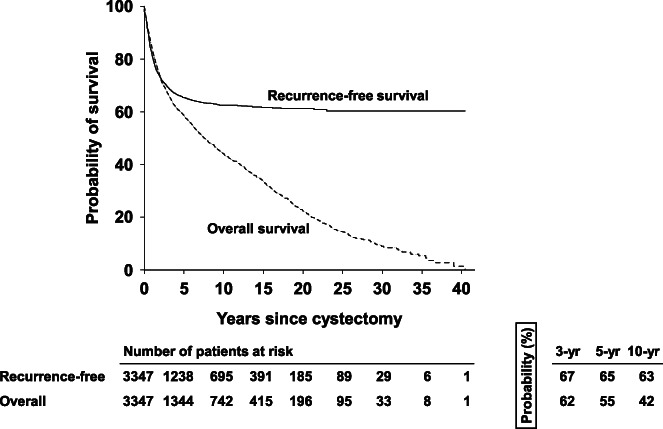
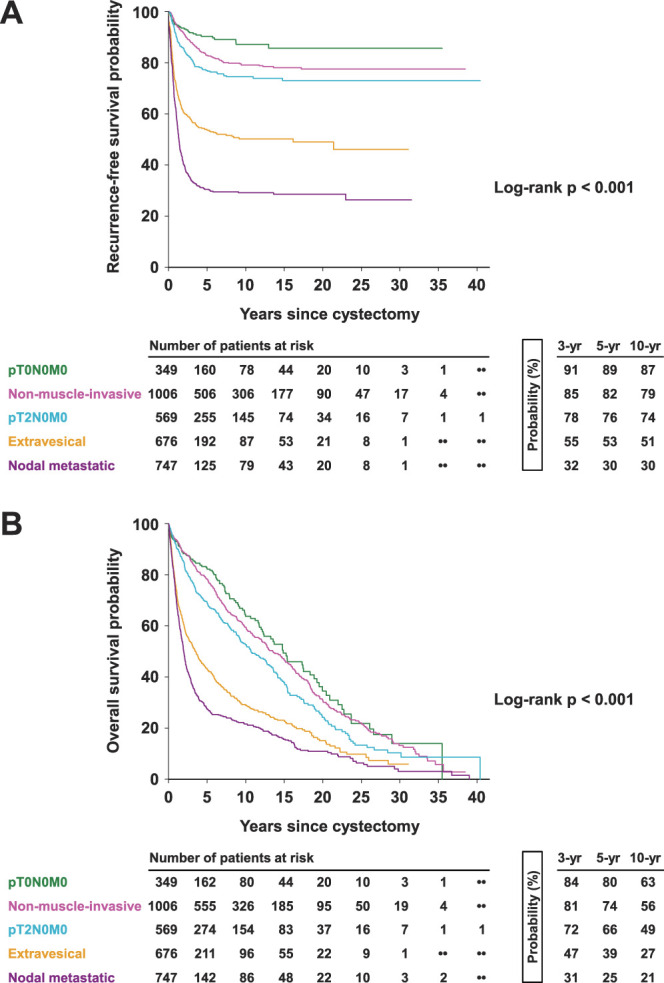
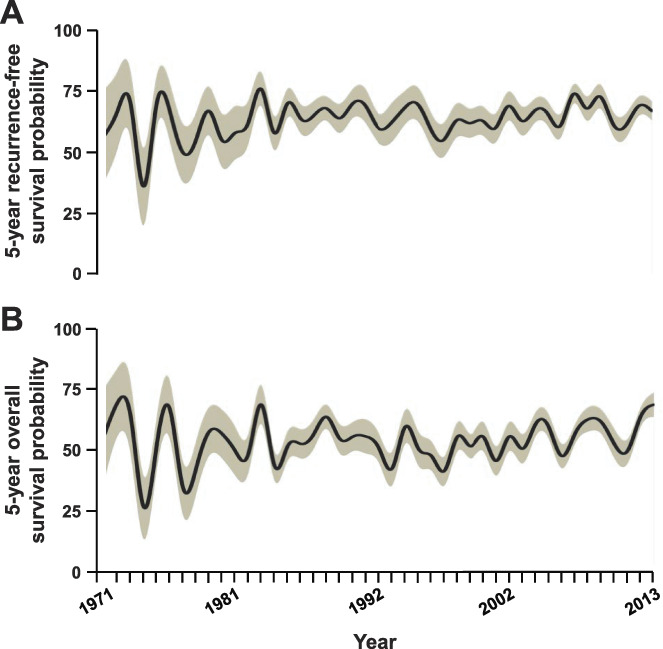
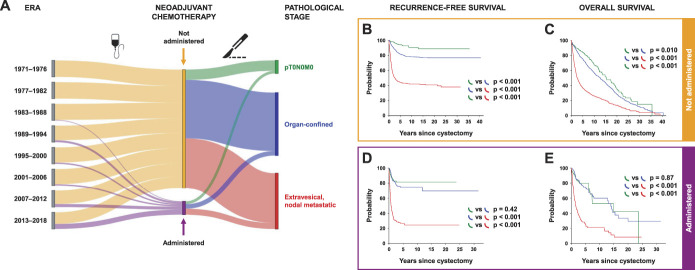
Results: In all, 70.9% of cases underwent open RC in the last decade, although trend for robot-assisted RC rose since 2009. While lymphadenectomy template remained consistent, nodal submission changed to anatomical packets in 2002 with increase in yield (p <0.001). Neoadjuvant chemotherapy (NAC) use increased with time with concomitant decrease in adjuvant chemotherapy; this was notable in the last decade (p <0.001) and coincided with improved pT0N0M0 rate (p=0.013). Median 5-year RFS and OS probabilities were 65% and 55%, respectively. Advanced stage, NAC, delay to RC, lymphovascular invasion and positive margins were associated with worse RFS (all, multivariable p <0.001). RFS remained stable over time (p=0.73) but OS improved (5-year probability, 1990-1999 51%, 2010-2018 62%; p=0.019). Among patients with extravesical and/or node-positive disease, those who received NAC had worse outcomes than those who directly underwent RC (p ≤0.001).
Conclusions: Despite perioperative and surgical advances, and improved pT0N0M0 rates, there has been no overall change in RFS trend following RC, although OS rates have improved. While patients who are downstaged with NAC derive great benefit, our real-world experience highlights the importance of preemptively identifying NAC nonresponders who may have worse post-RC outcomes.
Keywords: cystectomy; neoadjuvant therapy; prognosis; urinary bladder neoplasms; urinary diversion.
Figures
Comment in
-
Editorial Comment.J Urol. 2022 Feb;207(2):312-313. doi: 10.1097/JU.0000000000002242.01. Epub 2021 Nov 8. J Urol. 2022. PMID: 34994655 No abstract available.
References
-
- Abdollah F, Gandaglia G, Thuret R, et al. : Incidence, survival and mortality rates of stage-specific bladder cancer in United States: a trend analysis. Cancer Epidemiol 2013; 37: 219. - PubMed
-
- Morgan TM, Barocas DA, Keegan KA, et al. : Volume outcomes of cystectomy—is it the surgeon or the setting? J Urol 2012; 188: 2139. - PubMed
-
- Scarberry K, Berger NG, Scarberry KB, et al. : Improved surgical outcomes following radical cystectomy at high-volume centers influence overall survival. Urol Oncol 2018; 36: 308.e11. - PubMed
-
- Daneshmand S, Ahmadi H, Schuckman AK, et al. : Enhanced recovery protocol after radical cystectomy for bladder cancer. J Urol 2014; 192: 50. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
