

Early Local Therapy for the Primary Site in De Novo Stage IV Breast Cancer: Results of a Randomized Clinical Trial (EA2108)
- PMID: 34995128
- PMCID: PMC8937009
- DOI: 10.1200/JCO.21.02006
Early Local Therapy for the Primary Site in De Novo Stage IV Breast Cancer: Results of a Randomized Clinical Trial (EA2108)
Erratum in
-
Erratum.J Clin Oncol. 2022 Apr 20;40(12):1392. doi: 10.1200/JCO.22.00666. J Clin Oncol. 2022. PMID: 35427466 Free PMC article. No abstract available.
Abstract
Purpose: Distant metastases are present in 6% or more of patients with newly diagnosed breast cancer. In this context, locoregional therapy for the intact primary tumor has been hypothesized to improve overall survival (OS), but clinical trials have reported conflicting results.
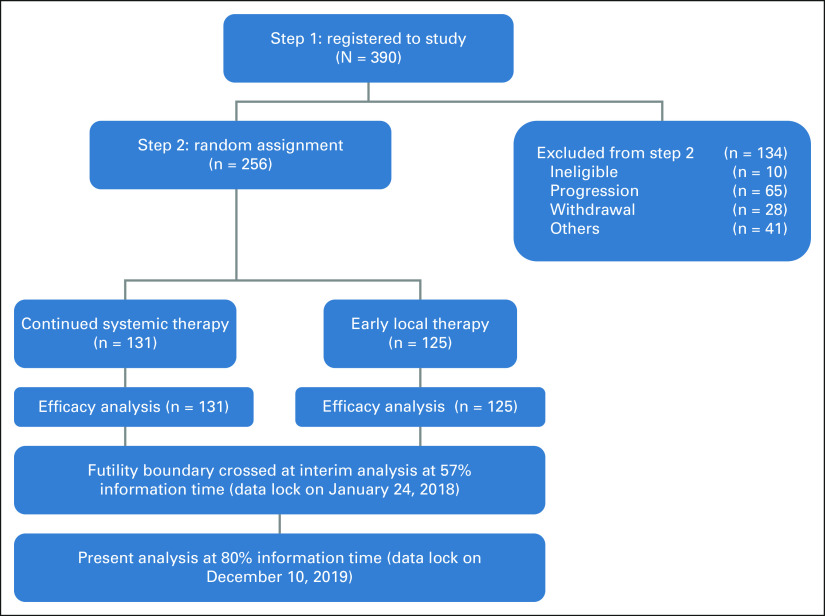
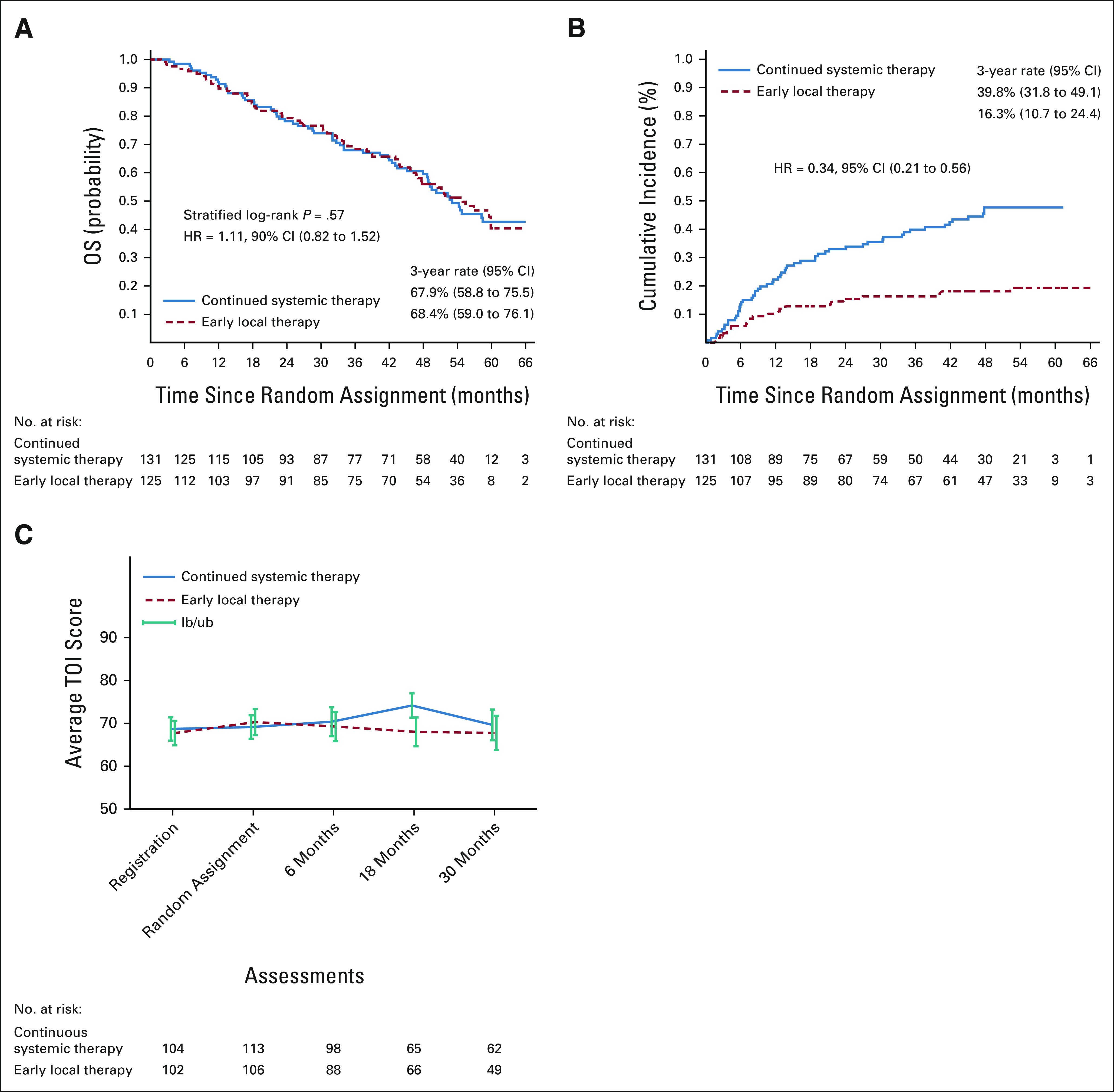
Methods: Women presenting with metastatic breast cancer and an intact primary tumor received systemic therapy for 4-8 months; if no disease progression occurred, they were randomly assigned to locoregional therapy for the primary site (surgery and radiotherapy per standards for nonmetastatic disease) or continuing sysmetic therapy. The primary end point was OS; locoregional control and quality of life were secondary end points. The trial design provided 85% power to detect a 19.3% absolute difference in the 3-year OS rate in randomly assigned patients. The stratified log-rank test and Cox proportional hazards model were used to compare OS between arms. Cumulative incidence of locoregional progression was compared using Gray's test. Quality-of-life assessment used standard instruments.
Results: Of 390 participants enrolled, 256 were randomly assigned: 131 to continued systemic therapy and 125 to early locoregional therapy. The 3-year OS was 67.9% without and 68.4% with early locoregional therapy (hazard ratio = 1.11; 90% CI, 0.82 to 1.52; P = .57). The median OS was 53.1 months (95% CI, 47.9 to not estimable) in the systemic therapy arm and 54.9 months (95% CI, 46.7 to not estimable) in the locoregional therapy arm. Locoregional progression was less frequent in those randomly assigned to locoregional therapy (3-year rate: 16.3% v 39.8%; P < .001). Quality-of-life measures were largely similar between arms.
Conclusion: Early locoregional therapy for the primary site did not improve survival in patients presenting with metastatic breast cancer. Although it was associated with improved locoregional control, this had no overall impact on quality of life.
Trial registration: ClinicalTrials.gov NCT01242800.
Conflict of interest statement
Figures
Comment in
-
Locoregional Therapy for Intact Primary Tumor in De Novo Stage IV Breast Cancer.J Clin Oncol. 2022 Nov 20;40(33):3897-3898. doi: 10.1200/JCO.22.00802. Epub 2022 Jul 12. J Clin Oncol. 2022. PMID: 35820106 No abstract available.
-
Early Local Therapy for the Primary Site in De Novo Stage IV Breast Cancer: Results of a Randomized Clinical Trial (EA2108).J Clin Oncol. 2022 Nov 20;40(33):3898. doi: 10.1200/JCO.22.00404. Epub 2022 Jul 12. J Clin Oncol. 2022. PMID: 35820107 No abstract available.
References
-
- Agarwal G, Pradeep PV, Aggarwal V, et al. Spectrum of breast cancer in Asian women World J Surg 311031–10402007 - PubMed
-
- Siegel RL, Miller KD, Jemal A.Cancer statistics, 2020 CA Cancer J Clin 707–302020 - PubMed
-
- Karnoub AE, Dash AB, Vo AP, et al. Mesenchymal stem cells within tumour stroma promote breast cancer metastasis Nature 449557–5632007 - PubMed
-
- Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer N Engl J Med 3451655–16592001 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- UG1 CA233320/CA/NCI NIH HHS/United States
- UG1 CA233329/CA/NCI NIH HHS/United States
- UG1 CA233234/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- UG1 CA232760/CA/NCI NIH HHS/United States
- UG1 CA233193/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1 CA233341/CA/NCI NIH HHS/United States
- UG1 CA233277/CA/NCI NIH HHS/United States
- UG1 CA189828/CA/NCI NIH HHS/United States
- UG1 CA189830/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- UG1 CA189953/CA/NCI NIH HHS/United States
- U10 CA180822/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
