

Impact of exposure time in awake prone positioning on clinical outcomes of patients with COVID-19-related acute respiratory failure treated with high-flow nasal oxygen: a multicenter cohort study
- PMID: 34996496
- PMCID: PMC8740872
- DOI: 10.1186/s13054-021-03881-2
Impact of exposure time in awake prone positioning on clinical outcomes of patients with COVID-19-related acute respiratory failure treated with high-flow nasal oxygen: a multicenter cohort study
Abstract
Background: In patients with COVID-19-related acute respiratory failure (ARF), awake prone positioning (AW-PP) reduces the need for intubation in patients treated with high-flow nasal oxygen (HFNO). However, the effects of different exposure times on clinical outcomes remain unclear. We evaluated the effect of AW-PP on the risk of endotracheal intubation and in-hospital mortality in patients with COVID-19-related ARF treated with HFNO and analyzed the effects of different exposure times to AW-PP.
Methods: This multicenter prospective cohort study in six ICUs of 6 centers in Argentine consecutively included patients > 18 years of age with confirmed COVID-19-related ARF requiring HFNO from June 2020 to January 2021. In the primary analysis, the main exposure was awake prone positioning for at least 6 h/day, compared to non-prone positioning (NON-PP). In the sensitivity analysis, exposure was based on the number of hours receiving AW-PP. Inverse probability weighting-propensity score (IPW-PS) was used to adjust the conditional probability of treatment assignment. The primary outcome was endotracheal intubation (ETI); and the secondary outcome was hospital mortality.
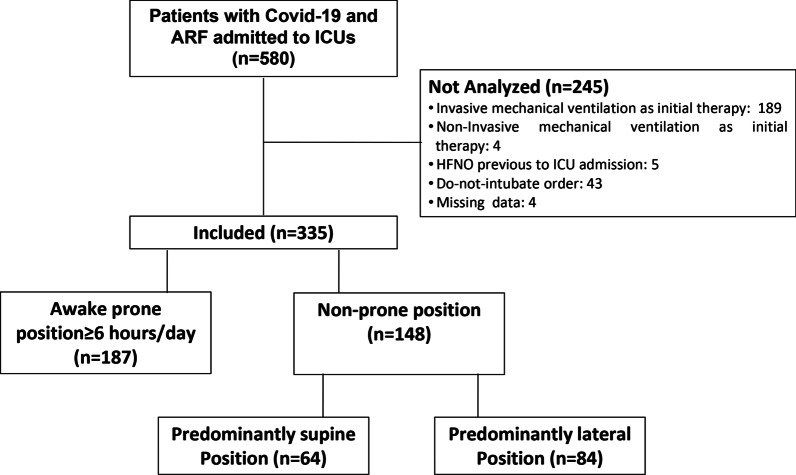
Results: During the study period, 580 patients were screened and 335 were included; 187 (56%) tolerated AW-PP for [median (p25-75)] 12 (9-16) h/day and 148 (44%) served as controls. The IPW-propensity analysis showed standardized differences < 0.1 in all the variables assessed. After adjusting for other confounders, the OR (95% CI) for ETI in the AW-PP group was 0.36 (0.2-0.7), with a progressive reduction in OR as the exposure to AW-PP increased. The adjusted OR (95% CI) for hospital mortality in the AW-PP group ≥ 6 h/day was 0.47 (0.19-1.31). The exposure to prone positioning ≥ 8 h/d resulted in a further reduction in OR [0.37 (0.17-0.8)].
Conclusion: In the study population, AW-PP for ≥ 6 h/day reduced the risk of endotracheal intubation, and exposure ≥ 8 h/d reduced the risk of hospital mortality.
Keywords: Acute respiratory failure; Awake; COVID-19; Endotracheal intubation; Mortality; Prone position.
© 2022. The Author(s).
Conflict of interest statement
AT is Consultant of Pfizer, Poliphor, MSD, Jansen OM Pharma. MB received lecture fees from Tecme S.A. and MEDIX Medical Devices S.R.L. Argentina. The rest of the authors declare that they have no competing interests.
Figures


References
-
- Karagiannidis C, Mostert C, Hentschker C, Voshaar T, Malzahn J, Schillinger G, et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study. Lancet Respir Med. 2020;8:853–862. doi: 10.1016/S2213-2600(20)30316-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
