

Associations of Neighborhood Socioeconomic Disadvantage With Chronic Conditions by Age, Sex, Race, and Ethnicity in a Population-Based Cohort
- PMID: 34996566
- PMCID: PMC8775356
- DOI: 10.1016/j.mayocp.2021.09.006
Associations of Neighborhood Socioeconomic Disadvantage With Chronic Conditions by Age, Sex, Race, and Ethnicity in a Population-Based Cohort
Abstract
Objective: To determine the association of socioeconomic status at the census block group level with chronic conditions and to determine whether the associations differ by age, sex, race, or ethnicity.
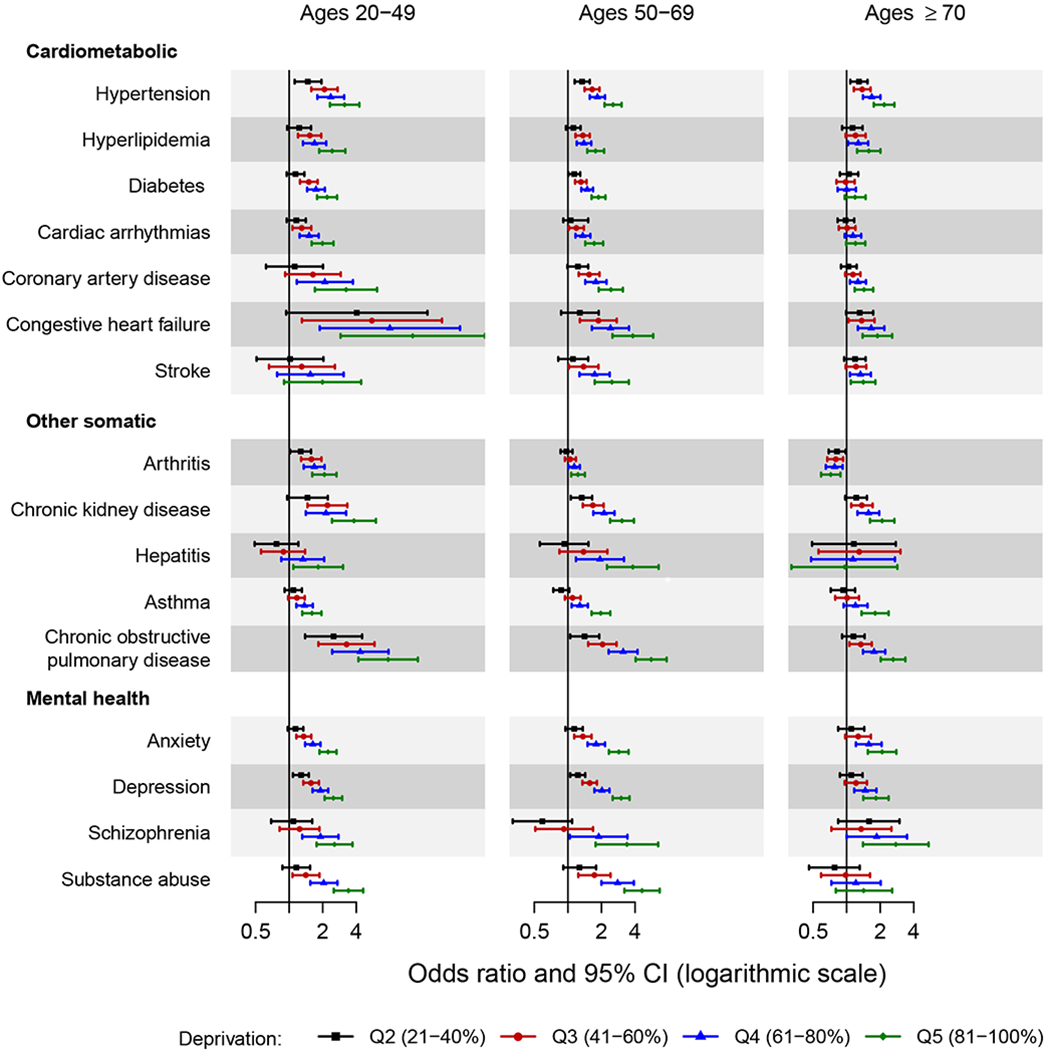
Methods: Adults aged 20 years and older on April 1, 2015, from 7 counties in southern Minnesota were identified using the Rochester Epidemiology Project records-linkage system. We estimated the prevalence of 19 chronic conditions (7 cardiometabolic, 7 other somatic, and 5 mental health conditions) at the individual level and a composite measure of neighborhood socioeconomic disadvantage (the area deprivation index [ADI]) at the census block group level (n=249).
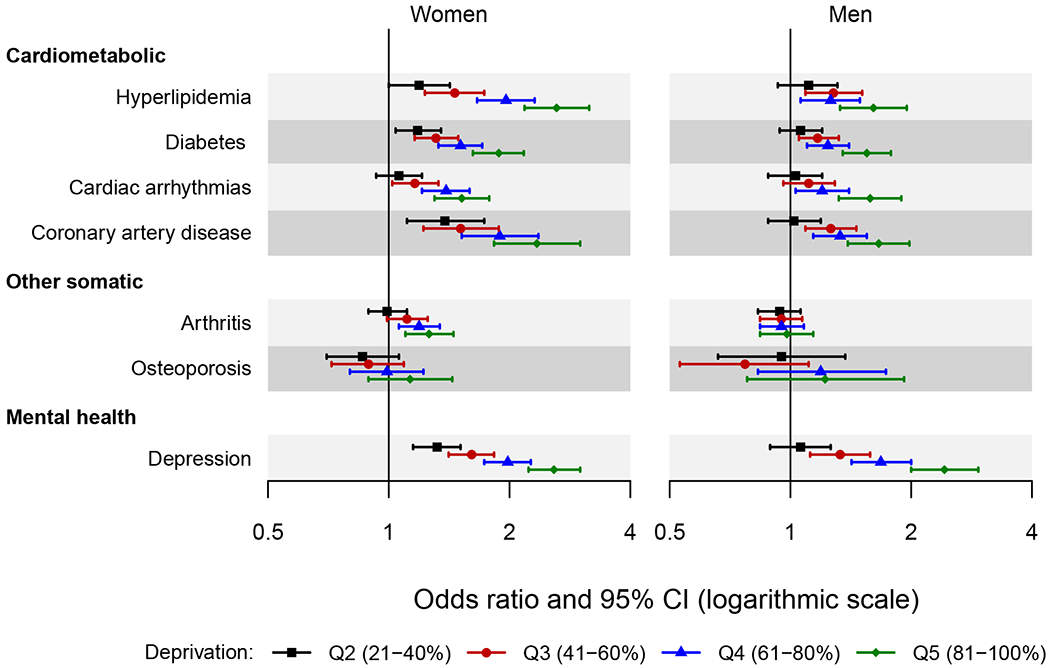
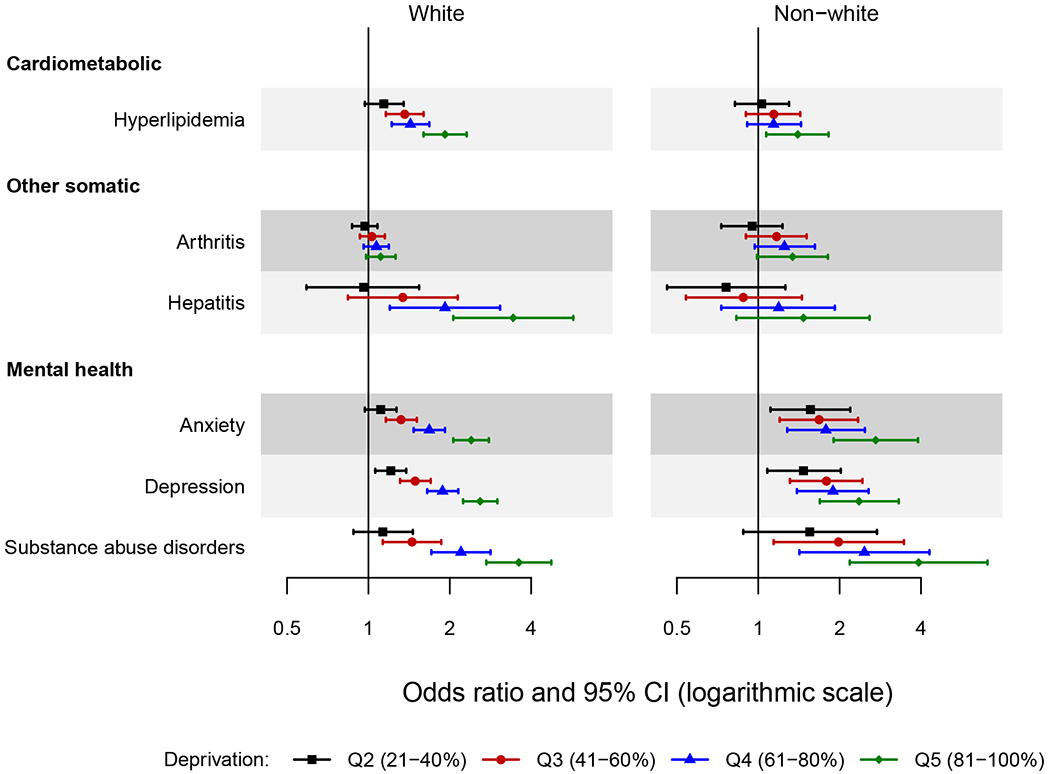
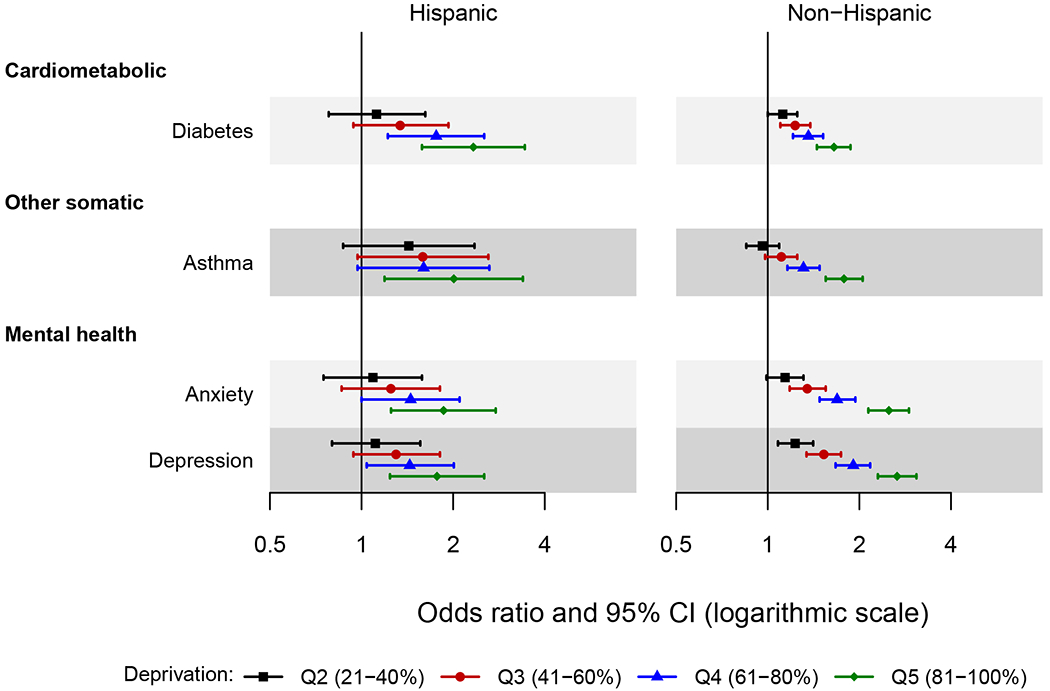
Results: Among the 197,578 persons in our study, 46.7% (92,373) were male, 49.5% (97,801) were aged 50 years and older, 12.3% (24,316) were of non-White race, and 5.3% (10,546) were Hispanic. The risk of most chronic conditions increased with increasing ADI. For each cardiometabolic condition and most other somatic and mental health conditions, the pattern of increasing risk across ADI quintiles was attenuated, or there was no association across quintiles of ADI in the oldest age group (aged ≥70 years). Stronger associations between ADI and several cardiometabolic, other somatic, and mental health conditions were observed in women.
Conclusion: Higher ADI was associated with increased risk of most chronic conditions, with more pronounced associations in younger persons. For some chronic conditions, the associations were stronger in women. Our findings underscore the importance of recognizing the overall and potentially differential impact of area-level deprivation on chronic disease outcomes for diverse populations.
Keywords: US Census; area deprivation index; chronic conditions; demographic variables; geocoding; socioeconomic status.
Copyright © 2021 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Leveraging Community Information to Improve Health Equity.Mayo Clin Proc. 2022 Jan;97(1):10-11. doi: 10.1016/j.mayocp.2021.11.013. Mayo Clin Proc. 2022. PMID: 34996541 No abstract available.
References
-
- Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. 2018;42(2):186–194. - PubMed
-
- Xu X, Mishra GD, Jones M. Evidence on multimorbidity from definition to intervention: an overview of systematic reviews. Ageing Res Rev. 2017;37:53–68. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
