

The association of lung function and pulmonary vasculature volume with cardiorespiratory fitness in the community
- PMID: 34996832
- PMCID: PMC9259762
- DOI: 10.1183/13993003.01821-2021
The association of lung function and pulmonary vasculature volume with cardiorespiratory fitness in the community
Abstract
Background: Cardiorespiratory fitness is not limited by pulmonary mechanical reasons in the majority of adults. However, the degree to which lung function contributes to exercise response patterns among ostensibly healthy individuals remains unclear.
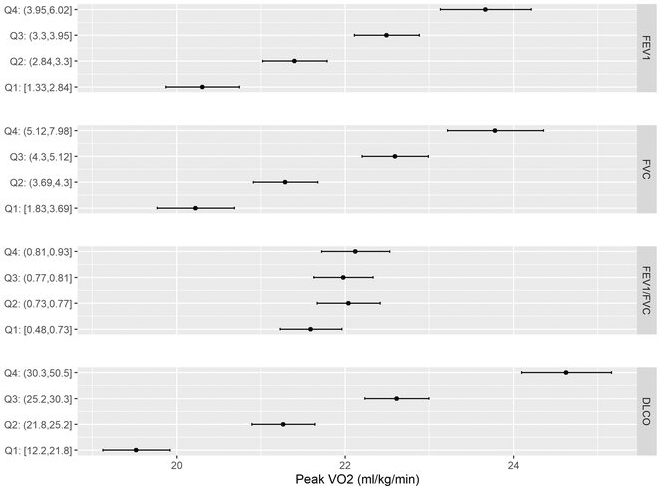
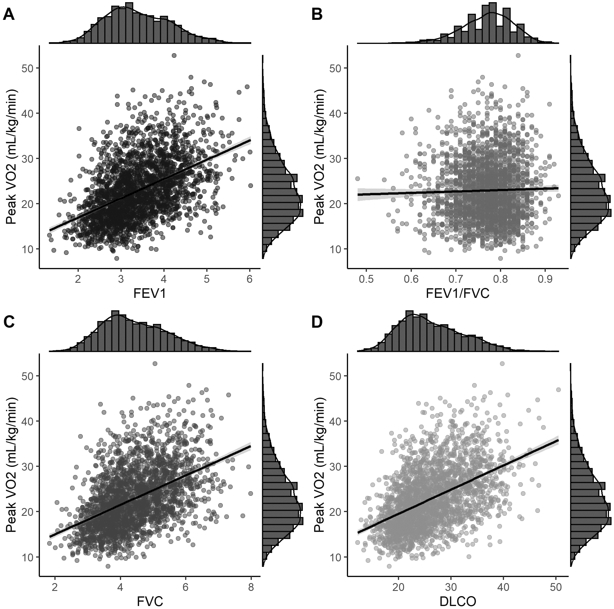
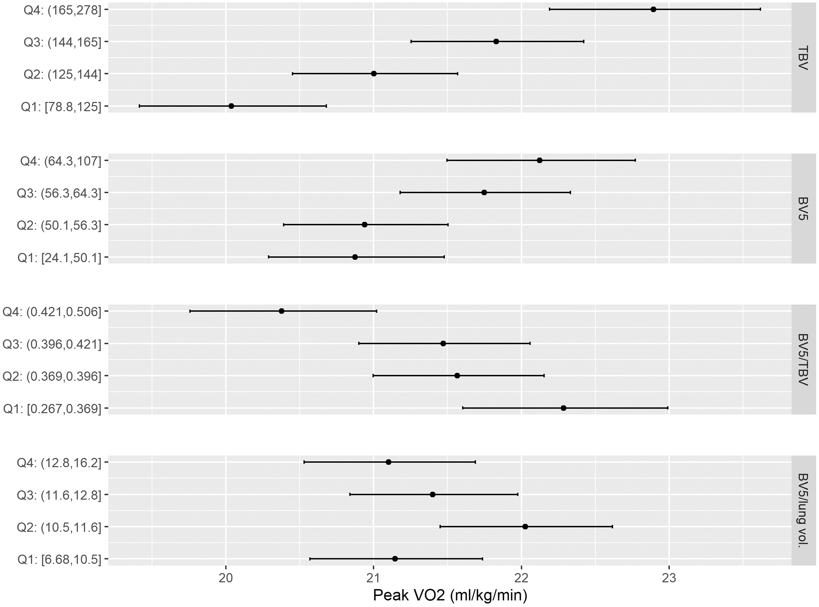
Methods: We examined 2314 Framingham Heart Study participants who underwent cardiopulmonary exercise testing (CPET) and pulmonary function testing. We investigated the association of forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC and diffusing capacity of the lung for carbon monoxide (D LCO) with the primary outcome of peak oxygen uptake (V'O2 ) along with other CPET parameters using multivariable linear regression. Finally, we investigated the association of total and peripheral pulmonary blood vessel volume with peak V'O2 .
Results: We found lower FEV1, FVC and D LCO were associated with lower peak V'O2 . For example, a 1 L lower FEV1 and FVC was associated with a 7.1% (95% CI 5.1-9.1%) and 6.0% (95% CI 4.3-7.7%) lower peak V'O2 , respectively. By contrast, FEV1/FVC was not associated with peak V'O2 . Lower lung function was associated with lower oxygen uptake efficiency slope, oxygen pulse slope, V'O2 at anaerobic threshold (AT), minute ventilation (V'E) at AT and breathing reserve. In addition, lower total and peripheral pulmonary blood vessel volume were associated with lower peak V'O2 .
Conclusions: In a large, community-based cohort of adults, we found lower FEV1, FVC and D LCO were associated with lower exercise capacity, as well as oxygen uptake efficiency slope and ventilatory efficiency. In addition, lower total and peripheral pulmonary blood vessel volume were associated with lower peak V'O2 . These findings underscore the importance of lung function and blood vessel volume as contributors to overall exercise capacity.
Copyright ©The authors 2022. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: J. McNeill has nothing to disclose. Conflict of interest: A. Chernofsky has nothing to disclose. Conflict of interest: M. Nayor reports grants from the NIH, during the conduct of the study. Conflict of interest: F.N. Rahaghi has nothing to disclose. Conflict of interest: R. San Jose Estepar has contracts with Lung Biotechnology, Insmed and Boehringer Ingelheim, receives consulting fees from Leuko Labs, and has stock options in Quantitative Imaging Solutions. Conflict of interest: G. Washko reports grants from the NIH, DoD, Boehringer Ingelheim, Janssen Pharmaceuticals, BTG Therapeutics, Pulmonx, Lung Biotechnology and Insmed; participation in advisory boards and consultancies for Boehringer Ingelheim, CSL Behring, Novartis, Phillips and Vertex Pharmaceuticals; is a co-founder and equity shareholder in Quantitative Imaging Solutions, a company that provides consulting services for image and data analytics; finally, the author's spouse works for Biogen. Conflict of interest: A. Synn reports grants from the American Lung Association and NHLBI, outside the submitted work. Conflict of interest: R.S. Vasan has nothing to disclose. Conflict of interest: G. O'Connor has nothing to disclose. Conflict of interest: M.G. Larson has nothing to disclose. Conflict of interest: J.E. Ho reports grants from the NIH/NHLBI, during the conduct of the study; research support from Gilead Sciences and Bayer AG, and research supplies from EcoNugenics, outside the submitted work. Conflict of interest: G.D. Lewis reports grants from Amgen, Cytokinetics, AstraZeneca, Applied Therapeutics and Sonivie, personal fees and other for advisory board work from American Regent, outside the submitted work.
Figures
References
-
- Mora S, Redberg RF, Cui Y, et al. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: a 20-year follow-up of the lipid research clinics prevalence study. JAMA. 2003;290(12):1600–1607. - PubMed
-
- Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–2035. - PubMed
-
- Clausen JSR, Marott JL, Holtermann A, Gyntelberg F, Jensen MT. Midlife Cardiorespiratory Fitness and the Long-Term Risk of Mortality: 46 Years of Follow-Up. J Am Coll Cardiol. 2018;72(9):987–995. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr., Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83(3):778–786. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL140224/HL/NHLBI NIH HHS/United States
- R01 HL131029/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- K23 HL136905/HL/NHLBI NIH HHS/United States
- R01 HL159514/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- R01 HL151841/HL/NHLBI NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- K23 HL138260/HL/NHLBI NIH HHS/United States
- F32 HL143819/HL/NHLBI NIH HHS/United States
- K24 HL153669/HL/NHLBI NIH HHS/United States
- R01 HL134893/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources