

Risk factors of flare in patients with systemic lupus erythematosus after glucocorticoids withdrawal. A systematic review and meta-analysis
- PMID: 34996857
- PMCID: PMC8744100
- DOI: 10.1136/lupus-2021-000603
Risk factors of flare in patients with systemic lupus erythematosus after glucocorticoids withdrawal. A systematic review and meta-analysis
Abstract
Objective: Glucocorticoids (GC) withdrawal is part of the targets in current recommendations for SLE, but relapse is the most worrying issue. We aimed to investigate the predictors for flare in patients with SLE after GC withdrawal.
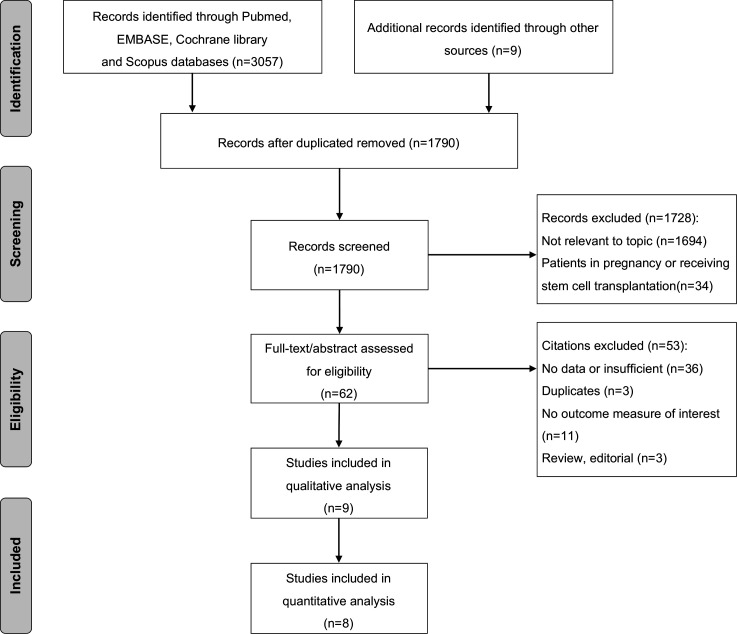
Methods: We systematically searched PubMed, EMBASE and Cochrane Library as well as Scopus databases up to 9 July 2021 for studies concerning predictive factors of relapses in patients with SLE after GC cessation. Pooled OR and 95% CI were combined using a random-effects or fixed-effects model.
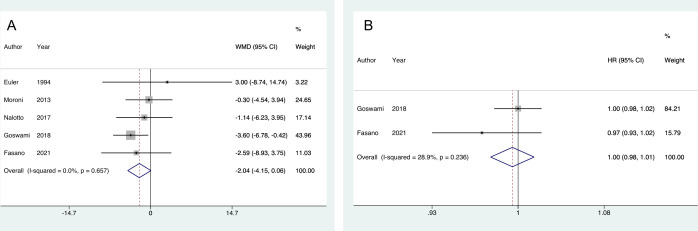
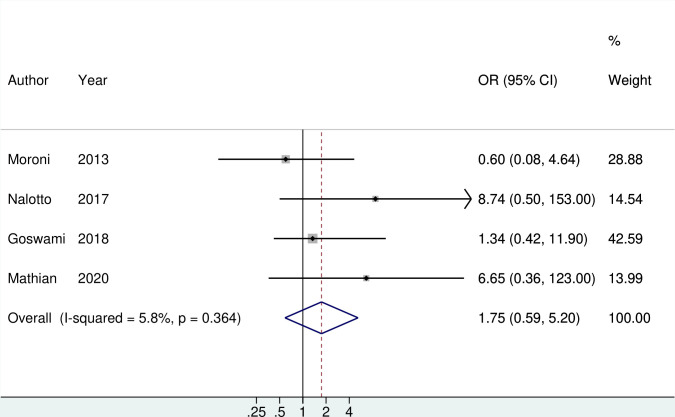
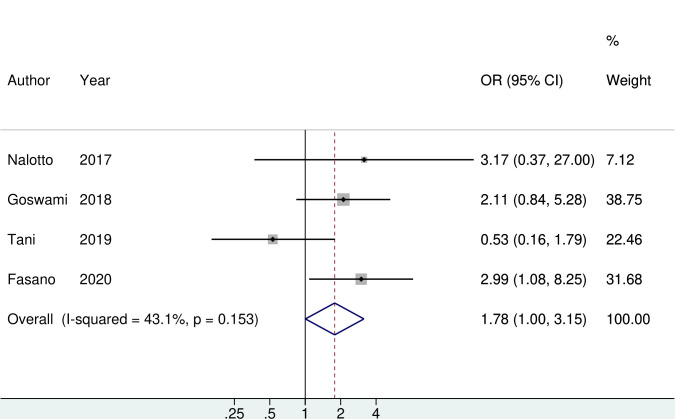
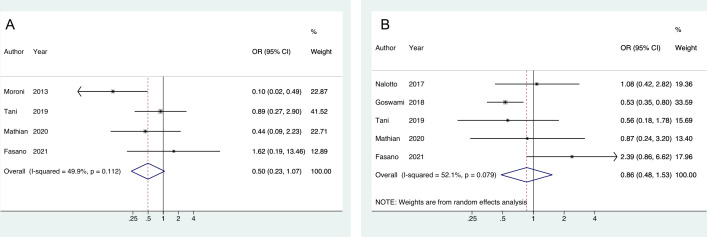
Results: 635 patients with SLE with GC discontinuation in 9 publications were eligible for the final analysis. Of them, 99.5% patients were in clinical remission before GC withdrawal. Serologically active yet clinically quiescent (SACQ) was associated with an increased risk of flare after GC withdrawal (OR 1.78, 95% CI (1.00 to 3.15)). Older age and concomitant use of hydroxychloroquine (HCQ) trended towards decreased risk of flare (weighted mean difference (WMD) -2.04, 95% CI (-4.15 to 0.06) for age and OR 0.50, 95% CI (0.23 to 1.07) for HCQ), yet not statistically significant. No significant association was observed regarding gender (pooled OR 1.75; 95% CI (0.59 to 5.20)), disease duration (WMD -11.91, 95% CI (-27.73 to 3.91)), remission duration (WMD -8.55, 95% CI (-33.33 to 16.23)), GC treatment duration (WMD -10.10, 95% CI (-64.09 to 43.88)), concomitant use of immunosuppressant (OR 0.86, 95% CI (0.48 to 1.53)).
Conclusion: Younger age and SACQ were potential risk factors of SLE flare among patients who discontinued GC. HCQ, but not immunosuppressant might prevent flare. GC withdrawal should be done with caution in this subgroup of patients.
Keywords: glucocorticoids; lupus erythematosus; lupus nephritis; systemic.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Low-dose glucocorticoids withdrawn in systemic lupus erythematosus: a desirable and attainable goal.Rheumatology (Oxford). 2022 Dec 23;62(1):181-189. doi: 10.1093/rheumatology/keac225. Rheumatology (Oxford). 2022. PMID: 35412598
-
Which patients with systemic lupus erythematosus in remission can withdraw low dose steroids? Results from a single inception cohort study.Lupus. 2021 May;30(6):991-997. doi: 10.1177/09612033211002269. Epub 2021 Mar 12. Lupus. 2021. PMID: 33709836
-
Low-dose glucocorticoids should be withdrawn or continued in systemic lupus erythematosus? A systematic review and meta-analysis on risk of flare and damage accrual.Rheumatology (Oxford). 2021 Dec 1;60(12):5517-5526. doi: 10.1093/rheumatology/keab149. Rheumatology (Oxford). 2021. PMID: 33576768
-
Prevalence and predictors of flare after immunosuppressant discontinuation in patients with systemic lupus erythematosus in remission.Rheumatology (Oxford). 2020 Jul 1;59(7):1591-1598. doi: 10.1093/rheumatology/kez422. Rheumatology (Oxford). 2020. PMID: 31642908
-
Glucocorticoid in systemic lupus erythematosus: the art beyond science.Expert Rev Clin Immunol. 2025 May;21(5):543-553. doi: 10.1080/1744666X.2025.2494654. Epub 2025 Apr 18. Expert Rev Clin Immunol. 2025. PMID: 40232132 Review.
Cited by
-
The dichotomy of glucocorticosteroid treatment in immune-inflammatory rheumatic diseases: an evidence-based perspective and insights from clinical practice.Reumatologia. 2023;61(4):283-293. doi: 10.5114/reum/170845. Epub 2023 Aug 31. Reumatologia. 2023. PMID: 37745141 Free PMC article. Review.
-
Clinical outcomes in lupus nephritis patients treated with belimumab in real-life setting: a retrospective comparative study in China.PeerJ. 2024 Sep 19;12:e18028. doi: 10.7717/peerj.18028. eCollection 2024. PeerJ. 2024. PMID: 39308826 Free PMC article.
-
Exploring the clinical characteristics and long-term outcome of serologically active clinically quiescent IgG4-related disease: knowledge from a prospective cohort.Clin Rheumatol. 2025 Jul;44(7):2929-2940. doi: 10.1007/s10067-025-07507-8. Epub 2025 May 30. Clin Rheumatol. 2025. PMID: 40445521
-
No clear influence of treatment escalation on flare prevention in serologically active clinically quiescent patients with systemic lupus erythematosus: a retrospective cohort study.Rheumatol Int. 2024 Nov;44(11):2411-2419. doi: 10.1007/s00296-024-05593-6. Epub 2024 Apr 26. Rheumatol Int. 2024. PMID: 38668884
-
TNFSF13B rs9514828 C>T Polymorphism is Associated with Incidence of Atherosclerosis and Therapeutic Outcomes in Patients with Systemic Lupus Erythematosus.Biologics. 2024 May 3;18:95-106. doi: 10.2147/BTT.S452792. eCollection 2024. Biologics. 2024. PMID: 38715569 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous