

Synchronous Occurrence of Advanced Gastric Carcinoma with Retroperitoneal Liposarcoma: A Case Report
- PMID: 34996885
- PMCID: PMC8754007
- DOI: 10.12659/AJCR.934586
Synchronous Occurrence of Advanced Gastric Carcinoma with Retroperitoneal Liposarcoma: A Case Report
Abstract
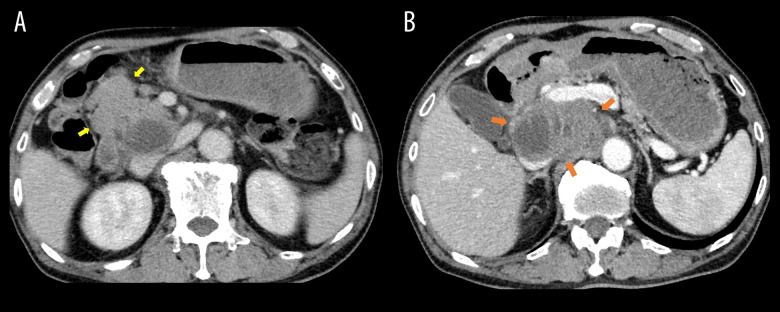
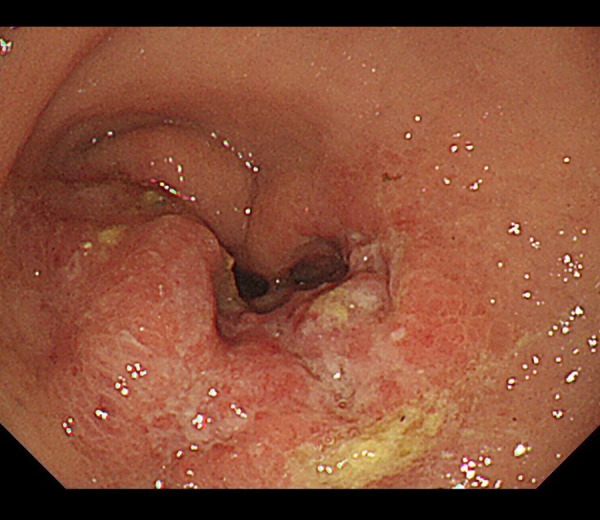
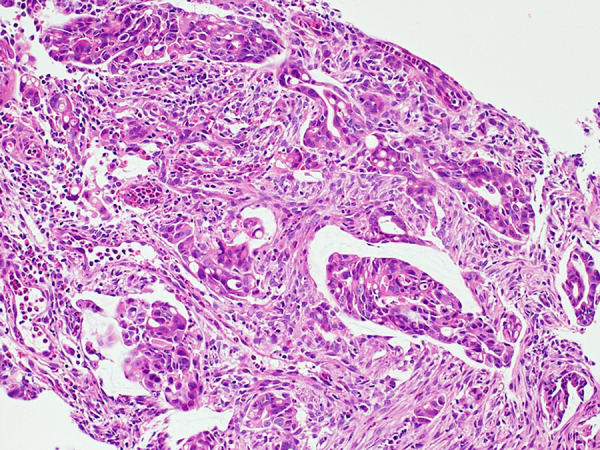
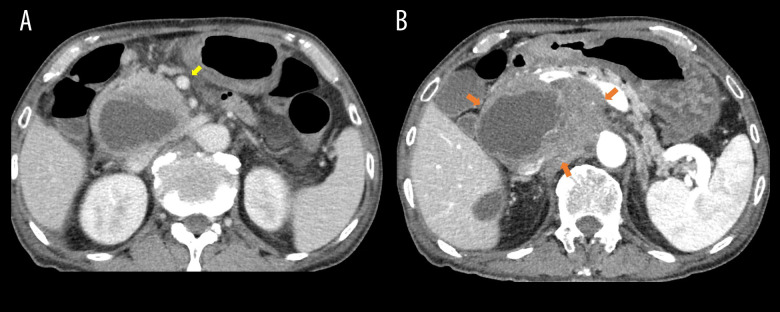
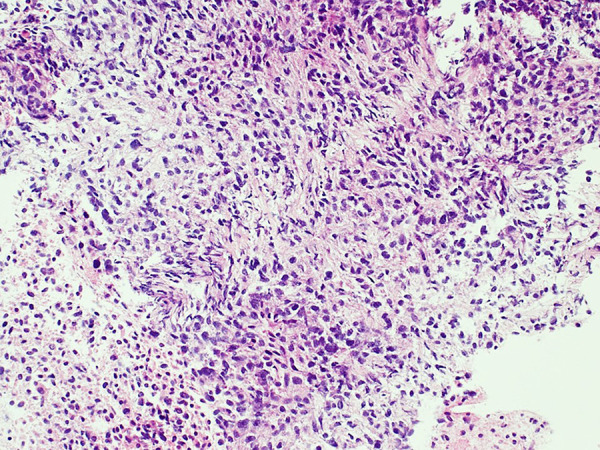
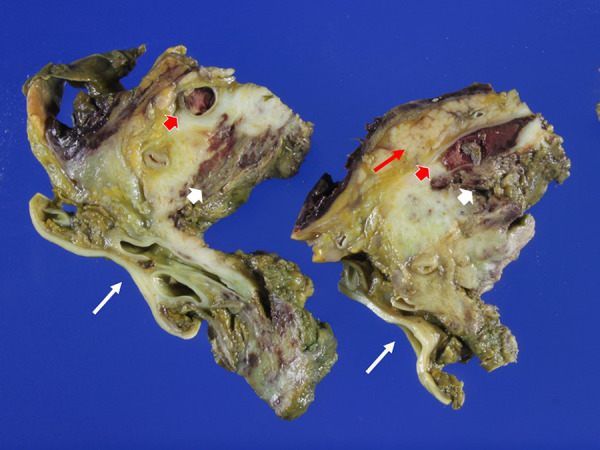
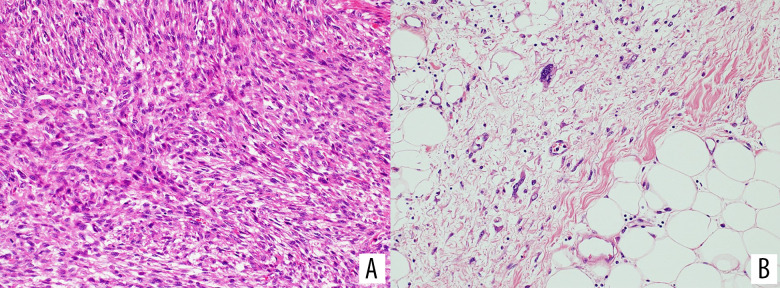
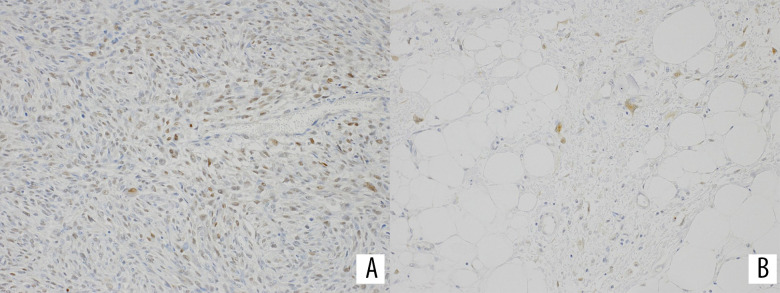
BACKGROUND Gastric carcinoma (GC) remains one of the most common and deadly neoplasms in the world. Liposarcoma (LPS) is the most common sarcoma of adults. However, synchronous or metachronous occurrence of GC with LPS seems to be very rare. Tumor staging and differential diagnosis with these cases are extremely difficult. CASE REPORT The patient was a man in his 70s, who reported anorexia and weight loss of 4 kg over 2 months. Gastroscopy demonstrated a large tumor of Borrmann type 3, of which histology was moderately to poorly differentiated adenocarcinoma. The clinical stage was initially defined as IVb due to a 11×6 cm retroperitoneal (RP) tumor. Despite chemotherapy for GC, the RP tumor rapidly enlarged. Endoscopic ultrasound-guided fine-needle aspiration biopsy showed that it was an undifferentiated sarcoma. He died of hepatorenal failure secondary to severe jaundice. The autopsy revealed a synchronous occurrence of GC and RP sarcoma. GC had no areas admixed with sarcoma. Histology of RP sarcoma showed that it mainly consisted of undifferentiated sarcoma and focally of well-differentiated LPS characterized by well-differentiated adipocytes admixed with scattered atypical stromal cells. The tumor cells in both areas were positive for MDM2 and CDK4 by immunohistochemistry. The diagnosis of the RP sarcoma was revised to dedifferentiated LPS. CONCLUSIONS There were no previous case reports of synchronous occurrence of GC with LPS in the English and Japanese literature. GC and LPS pose challenging problems in their diagnoses, staging, and treatments when they occur synchronously or metachronously.
Conflict of interest statement
Figures
Similar articles
-
Dedifferentiated liposarcoma with "homologous" lipoblastic (pleomorphic liposarcoma-like) differentiation: clinicopathologic and molecular analysis of a series suggesting revised diagnostic criteria.Am J Surg Pathol. 2010 Aug;34(8):1122-31. doi: 10.1097/PAS.0b013e3181e5dc49. Am J Surg Pathol. 2010. PMID: 20588177
-
Overlapping features between dedifferentiated liposarcoma and undifferentiated high-grade pleomorphic sarcoma.Am J Surg Pathol. 2009 Nov;33(11):1594-600. doi: 10.1097/PAS.0b013e3181accb01. Am J Surg Pathol. 2009. PMID: 19574885
-
Retroperitoneal liposarcoma with pancreatic metastasis and gastric cancer: a case report.Clin J Gastroenterol. 2023 Apr;16(2):164-170. doi: 10.1007/s12328-022-01742-1. Epub 2022 Dec 19. Clin J Gastroenterol. 2023. PMID: 36534319
-
Diagnostically Challenging "Fatty" Retroperitoneal Tumors.Surg Pathol Clin. 2015 Sep;8(3):375-97. doi: 10.1016/j.path.2015.05.008. Surg Pathol Clin. 2015. PMID: 26297062 Review.
-
Gastrointestinal Stromal Tumor (GIST) and Synchronous Intra-Abdominal Liposarcoma: A Report of Two Rare Cases and Literature Review.Int J Surg Oncol. 2021 Sep 1;2021:2626635. doi: 10.1155/2021/2626635. eCollection 2021. Int J Surg Oncol. 2021. PMID: 34518784 Free PMC article. Review.
Cited by
-
Synchronous retroperitoneal liposarcoma and gastric adenocarcinoma: A rare case report.Radiol Case Rep. 2024 Aug 23;19(11):5158-5163. doi: 10.1016/j.radcr.2024.07.142. eCollection 2024 Nov. Radiol Case Rep. 2024. PMID: 39263512 Free PMC article.
-
Synchronous occurrence of small cell lung cancer and primary rectal dedifferentiated liposarcoma with osteosarcomatous differentiation: A rare case report.Medicine (Baltimore). 2023 Sep 29;102(39):e35465. doi: 10.1097/MD.0000000000035465. Medicine (Baltimore). 2023. PMID: 37773783 Free PMC article.
References
-
- Fletcher CDM, Baldini EH, Blay JY, et al. Soft Tissue and Bone Tumours. 5th ed. The WHO Classification of Tumours Editorial Board. IARC; Lyon (France): 2020. Soft tissue tumors: Introduction In WHO Classification of Tumours.
-
- Japanese Orthopaedic Association . Japanese Orthopaedic Association (JOA) Clinical Practice Guidelines on the Management of Soft Tissue Tumors 2020 third ed. (JOA); Nankodo, Tokyo: 2020. - PubMed
-
- National Cancer Center for Cancer Control and Information Service Monitoring of cancer incidence Japan. Available at: https://ganjoho.jp/public/qa_links/report/ncr/monitoring.html [in Japanese]
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2018;68:394–424. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
