

Personalizing cholesterol treatment recommendations for primary cardiovascular disease prevention
- PMID: 34996943
- PMCID: PMC8742083
- DOI: 10.1038/s41598-021-03796-6
Personalizing cholesterol treatment recommendations for primary cardiovascular disease prevention
Abstract
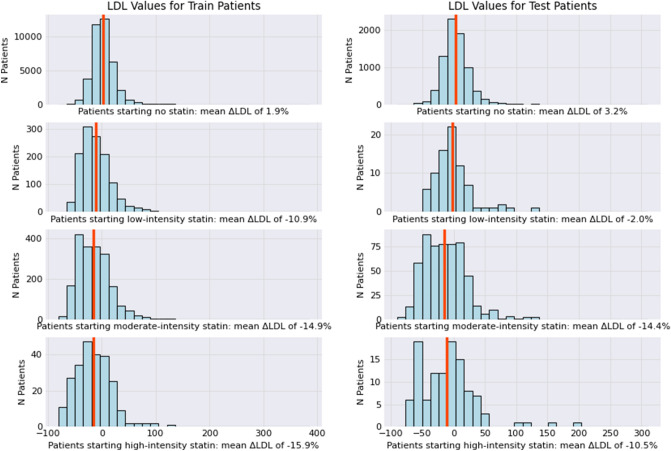
Statin therapy is the cornerstone of preventing atherosclerotic cardiovascular disease (ASCVD), primarily by reducing low density lipoprotein cholesterol (LDL-C) levels. Optimal statin therapy decisions rely on shared decision making and may be uncertain for a given patient. In areas of clinical uncertainty, personalized approaches based on real-world data may help inform treatment decisions. We sought to develop a personalized statin recommendation approach for primary ASCVD prevention based on historical real-world outcomes in similar patients. Our retrospective cohort included adults from a large Northern California electronic health record (EHR) aged 40-79 years with no prior cardiovascular disease or statin use. The cohort was split into training and test sets. Weighted-K-nearest-neighbor (wKNN) regression models were used to identify historical EHR patients similar to a candidate patient. We modeled four statin decisions for each patient: none, low-intensity, moderate-intensity, and high-intensity. For each candidate patient, the algorithm recommended the statin decision that was associated with the greatest percentage reduction in LDL-C after 1 year in similar patients. The overall cohort consisted of 50,576 patients (age 54.6 ± 9.8 years) with 55% female, 48% non-Hispanic White, 32% Asian, and 7.4% Hispanic patients. Among 8383 test-set patients, 52%, 44%, and 4% were recommended high-, moderate-, and low-intensity statins, respectively, for a maximum predicted average 1-yr LDL-C reduction of 16.9%, 20.4%, and 14.9%, in each group, respectively. Overall, using aggregate EHR data, a personalized statin recommendation approach identified the statin intensity associated with the greatest LDL-C reduction in historical patients similar to a candidate patient. Recommendations included low- or moderate-intensity statins for maximum LDL-C lowering in nearly half the test set, which is discordant with their expected guideline-based efficacy. A data-driven personalized statin recommendation approach may inform shared decision making in areas of uncertainty, and highlight unexpected efficacy-effectiveness gaps.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Grundy SM, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: Executive summary: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2019;73:3168–3209. doi: 10.1016/j.jacc.2018.11.002. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
