

Targeting immunoliposomes to EGFR-positive glioblastoma
- PMID: 34998092
- PMCID: PMC8741448
- DOI: 10.1016/j.esmoop.2021.100365
Targeting immunoliposomes to EGFR-positive glioblastoma
Abstract
Background: We assessed the capacity of epidermal growth factor receptor (EGFR)-targeted immunoliposomes to deliver cargo to brain tumor tissue in patients with relapsed glioblastoma harboring an EGFR amplification. We aimed to assess the tolerability and effectiveness of anti-EGFR immunoliposomes loaded with doxorubicin (anti-EGFR ILs-dox) in glioblastoma multiforme patients.
Patients and methods: Patients with EGFR-amplified, relapsed glioblastoma were included in this phase I pharmacokinetic trial. Patients received up to four cycles of anti-EGFR ILs-dox. Twenty-four hours later, plasma and cerebrospinal fluid (CSF) samples were obtained. In addition, we also treated three patients with anti-EGFR ILs-dox before resection of their relapsed glioblastoma. Doxorubicin concentrations were measured in plasma, CSF, and tumor tissue. Safety and efficacy parameters were also obtained.
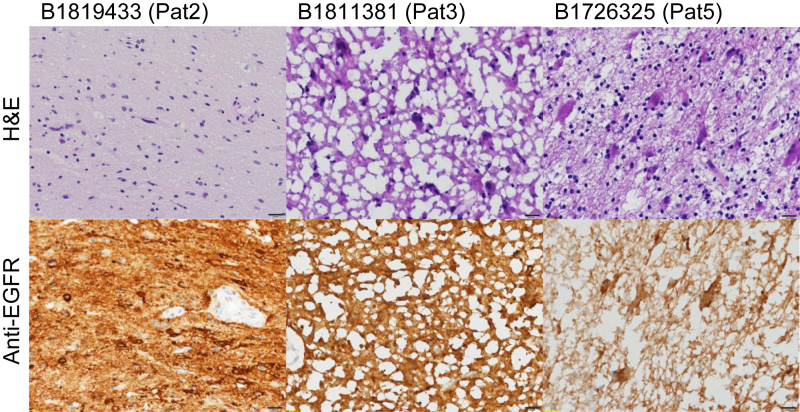
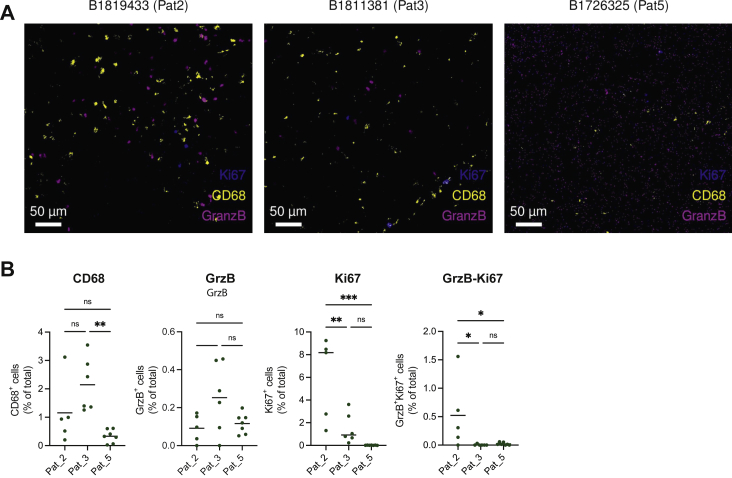
Results: There were no or negligible levels of doxorubicin found in the CSF demonstrating that anti-EGFR ILs-dox are not able to cross the blood-brain barrier (BBB). However, significant levels were detected in glioblastoma tissue 24 h after the application, indicating that the disruption of BBB integrity present in high-grade gliomas might enable liposome delivery into tumor tissue. No new safety issues were observed. The median progression-free survival was 1.5 months and the median overall survival was 8 months. One patient undergoing surgery had a very long remission suggesting that neoadjuvant administration may have a positive effect on outcome.
Conclusions: We clearly demonstrate that anti-EGFR-immunoliposomes can be targeted to EGFR-amplified glioblastoma and cargo-in this case doxorubicin-can be delivered, although these immunoliposomes do not cross the intact BBB. (The GBM-LIPO trial was registered as NCT03603379).
Keywords: blood–brain barrier; cerebrospinal fluid; nanomedicine; pharmacokinetic; targeted therapy.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure HL received travel grants and consultant fees from Bristol-Myers Squibb (BMS) and Merck, Sharp and Dohme (MSD); and research support from BMS, Novartis, GlycoEra, and Palleon Pharmaceuticals. BK has received research support from Roche and Abbvie; and consultant fees from Astellas and Riemser. The remaining authors have declared no conflicts of interest.
Figures
References
-
- Stupp R., Mason W.P., van den Bent M.J., et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Wirsching H.G., Galanis E., Weller M. Glioblastoma. Handb Clin Neurol. 2016;134:381–397. - PubMed
-
- Roth P., Hottinger A.F., Hundsberger T., et al. A contemporary perspective on the diagnosis and treatment of diffuse gliomas in adults. Swiss Med Wkly. 2020;150:w20256. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
