

Triage and monitoring of COVID-19 patients in intensive care using unsupervised machine learning
- PMID: 34998220
- PMCID: PMC8719000
- DOI: 10.1016/j.compbiomed.2021.105192
Triage and monitoring of COVID-19 patients in intensive care using unsupervised machine learning
Abstract
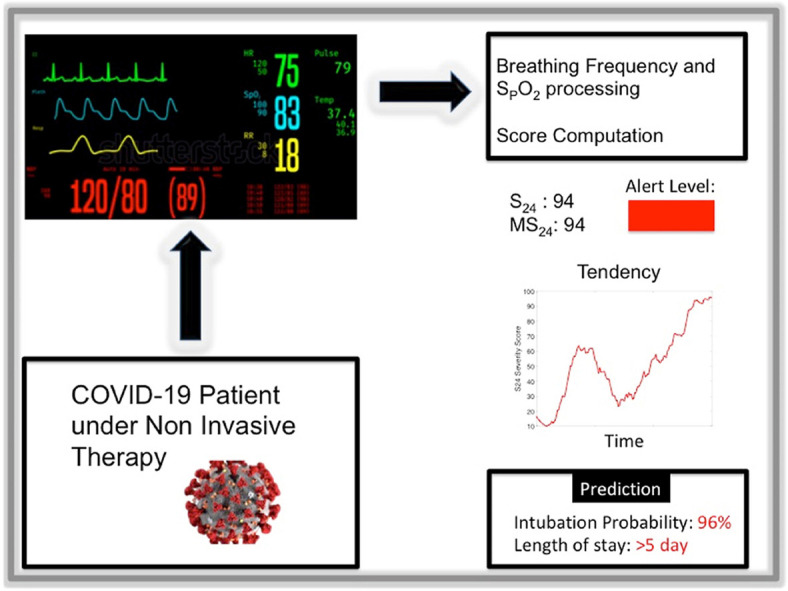
Background: We designed an algorithm to assess COVID-19 patients severity and dynamic intubation needs and predict their length of stay using the breathing frequency (BF) and oxygen saturation (SpO2) signals.
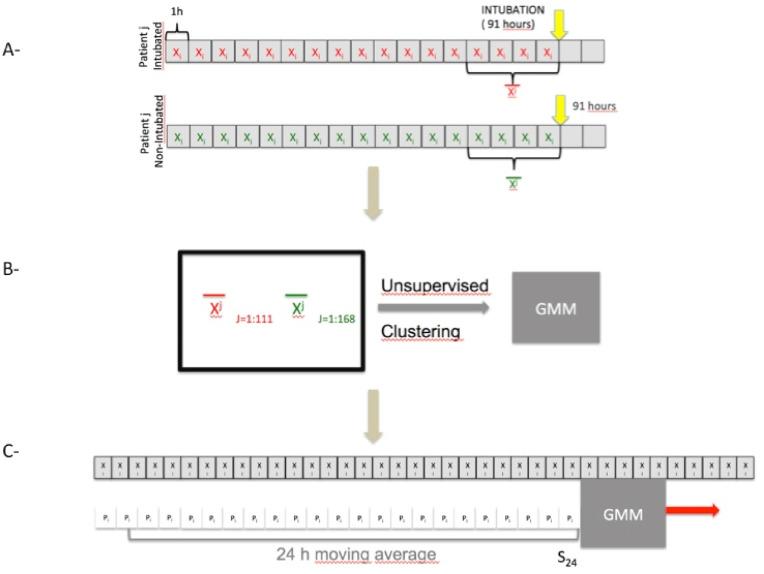
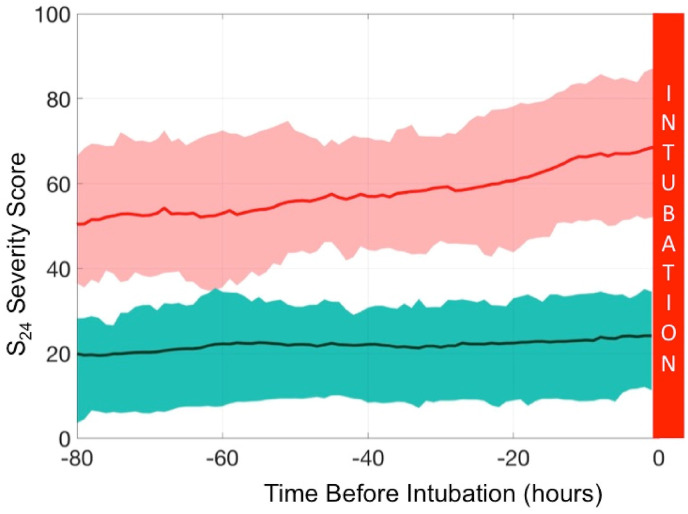
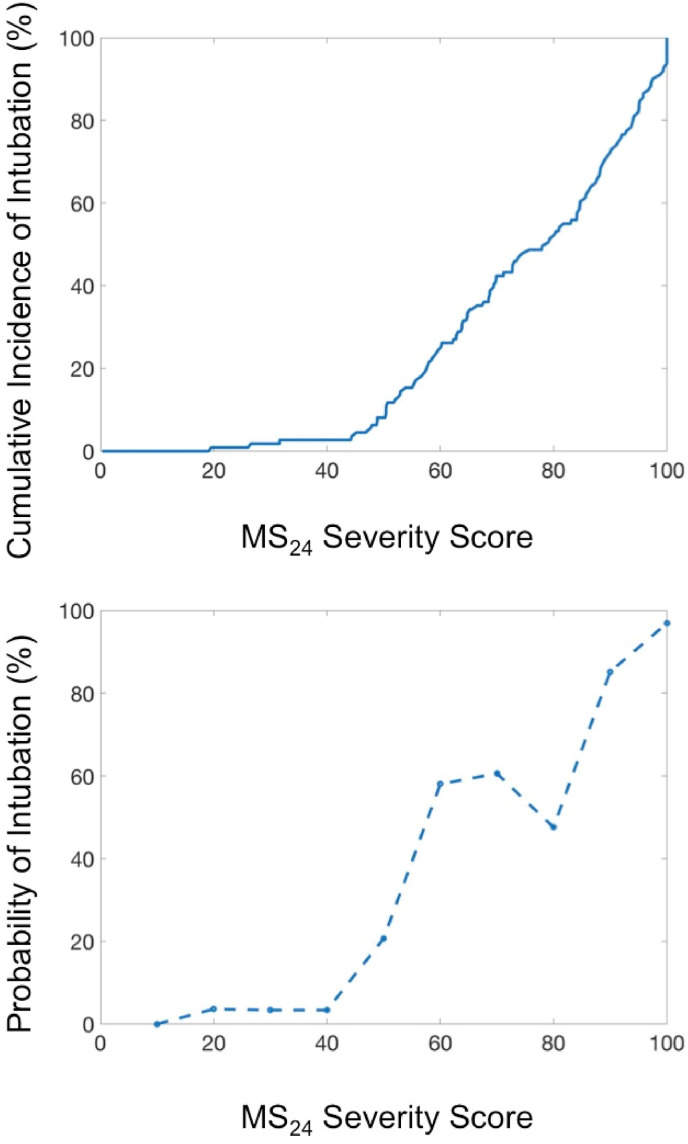
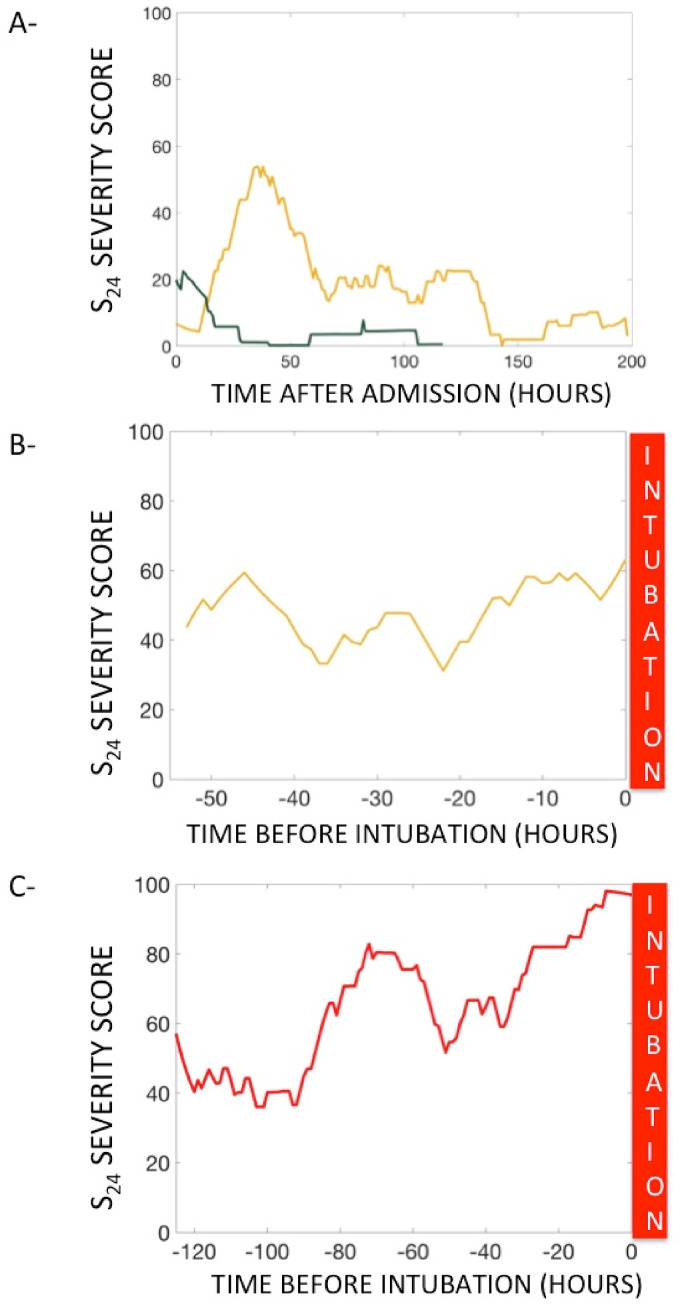
Methods: We recorded the BF and SpO2 signals for confirmed COVID-19 patients admitted to the ICU of a teaching hospital during both the first and subsequent outbreaks of the pandemic in France. An unsupervised machine-learning algorithm (the Gaussian mixture model) was applied to the patients' data for clustering. The algorithm's robustness was ensured by comparing its results against actual intubation rates. We predicted intubation rates using the algorithm every hour, thus conducting a severity evaluation. We designed a S24 severity score that represented the patient's severity over the previous 24 h; the validity of MS24, the maximum S24 score, was checked against rates of intubation risk and prolonged ICU stay.
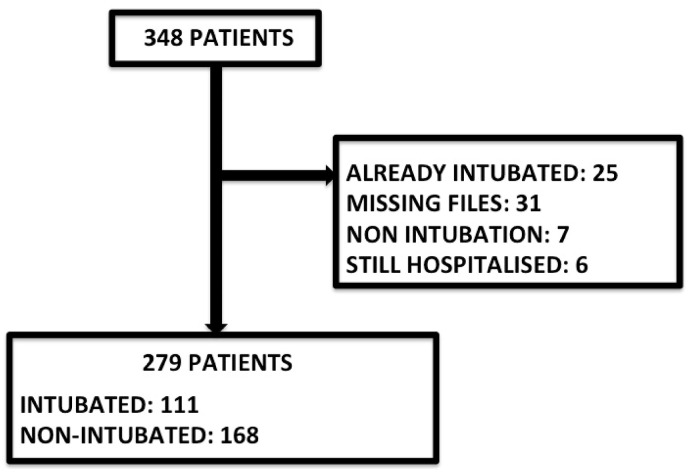
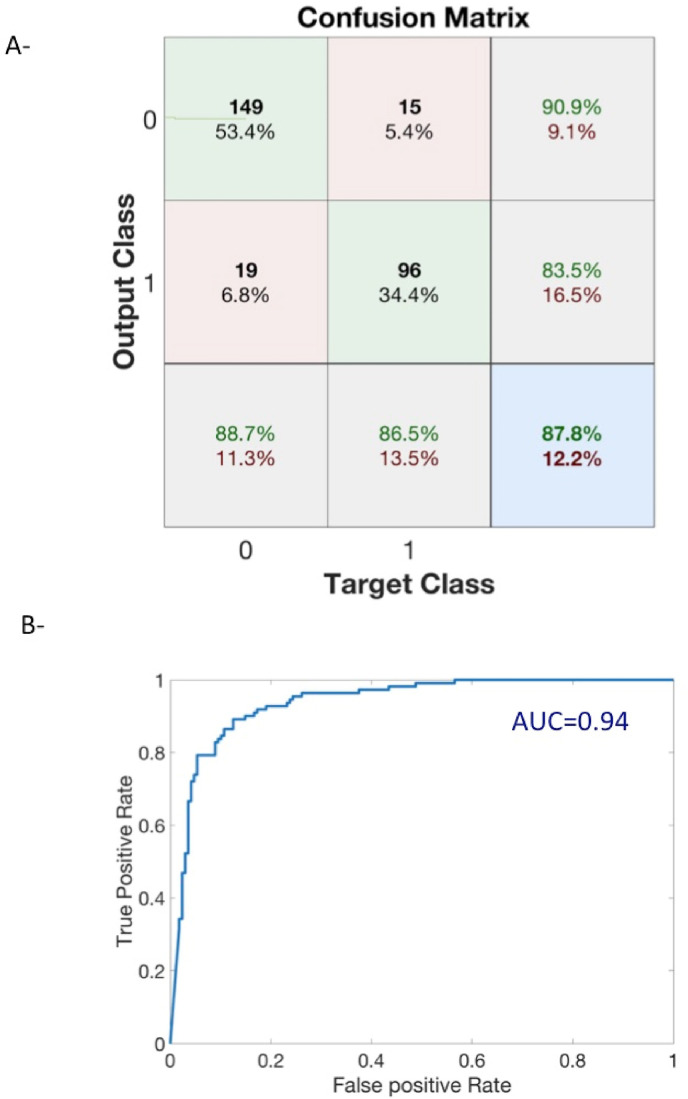
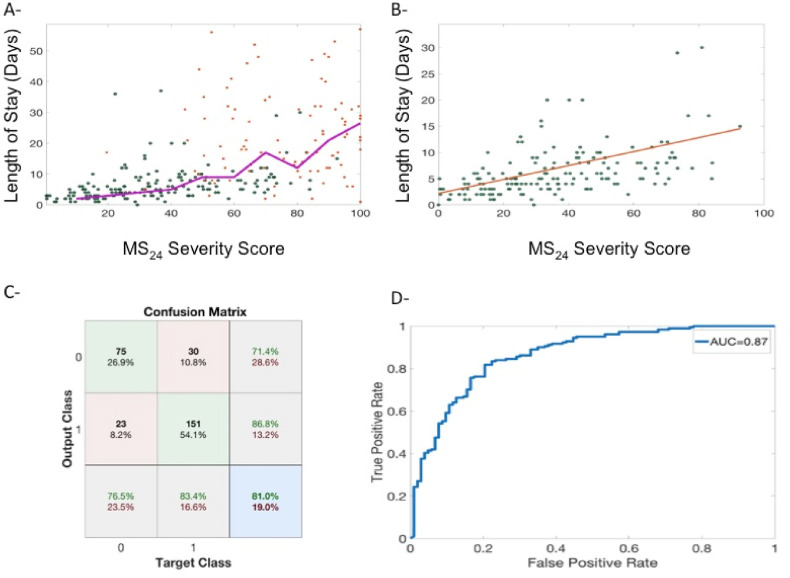
Results: Our sample included 279 patients. . The unsupervised clustering had an accuracy rate of 87.8% for intubation recognition (AUC = 0.94, True Positive Rate 86.5%, true Negative Rate 90.9%). The S24 score of intubated patients was significantly higher than that of non-intubated patients at 48 h before intubation. The MS24 score allowed for the distinguishing between three severity levels with an increased risk of intubation: green (3.4%), orange (37%), and red (77%). A MS24 score over 40 was highly predictive of an ICU stay greater than 5 days at an accuracy rate of 81.0% (AUC = 0.87).
Conclusions: Our algorithm uses simple signals and seems to efficiently visualize the patients' respiratory situations, meaning that it has the potential to assist staffs' in decision-making. Additionally, real-time computation is easy to implement.
Keywords: Artificial intelligence; COVID-19; Intubation; Monitoring; Prediction.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
None Declared.
Figures
References
-
- Maves R.C., Downar J., Dichter J.R., Hick J.L., Devereaux A., Geiling J.A., Kissoon N., Hupert N., Niven A.S., King M.A., Rubinson L.L., Hanfling D., Hodge J.G., Marshall M.F., Fischkoff K., Evans L.E., Tonelli M.R., Wax R.S., Seda G., Parrish J.S., Truog R.D., Sprung C.L., Christian M.D. Triage of scarce critical care resources in COVID-19 an implementation guide for regional allocation: an expert panel report of the task force for mass critical care and the American college of chest physicians. Chest. 2020;158:212–225. doi: 10.1016/j.chest.2020.03.063. - DOI - PMC - PubMed
-
- Xia J., Zhang Y., Ni L., Chen L., Zhou C., Gao C., Wu X., Duan J., Xie J., Guo Q., Zhao J., Hu Y., Cheng Z., Zhan Q. High-flow nasal oxygen in coronavirus disease 2019 patients with acute hypoxemic respiratory failure: a multicenter, retrospective cohort study. Crit. Care Med. 2020;48 doi: 10.1097/CCM.0000000000004558. - DOI - PMC - PubMed
-
- Demoule A., Vieillard Baron A., Darmon M., Beurton A., Géri G., Voiriot G., Dupont T., Zafrani L., Girodias L., Labbé V., Dres M., Fartoukh M., Azoulay E. High-flow nasal cannula in critically III patients with severe COVID-19. Am. J. Respir. Crit. Care Med. 2020;202:1039–1042. doi: 10.1164/rccm.202005-2007LE. - DOI - PMC - PubMed
-
- Calligaro G.L., Lalla U., Audley G., Gina P., Miller M.G., Mendelson M., Dlamini S., Wasserman S., Meintjes G., Peter J., Levin D., Dave J.A., Ntusi N., Meier S., Little F., Moodley D.L., Louw E.H., Nortje A., Parker A., Taljaard J.J., Allwood B.W., Dheda K., Koegelenberg C.F.N. The utility of high-flow nasal oxygen for severe COVID-19 pneumonia in a resource-constrained setting: a multi-centre prospective observational study. EClinicalMedicine. 2020;28 doi: 10.1016/j.eclinm.2020.100570. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
