

Durability of Clinical and Quality-of-Life Outcomes of Closed-Loop Spinal Cord Stimulation for Chronic Back and Leg Pain: A Secondary Analysis of the Evoke Randomized Clinical Trial
- PMID: 34998276
- PMCID: PMC8742908
- DOI: 10.1001/jamaneurol.2021.4998
Durability of Clinical and Quality-of-Life Outcomes of Closed-Loop Spinal Cord Stimulation for Chronic Back and Leg Pain: A Secondary Analysis of the Evoke Randomized Clinical Trial
Erratum in
-
Error in Figure.JAMA Neurol. 2022 Apr 1;79(4):420. doi: 10.1001/jamaneurol.2022.0022. JAMA Neurol. 2022. PMID: 35156999 Free PMC article. No abstract available.
Abstract
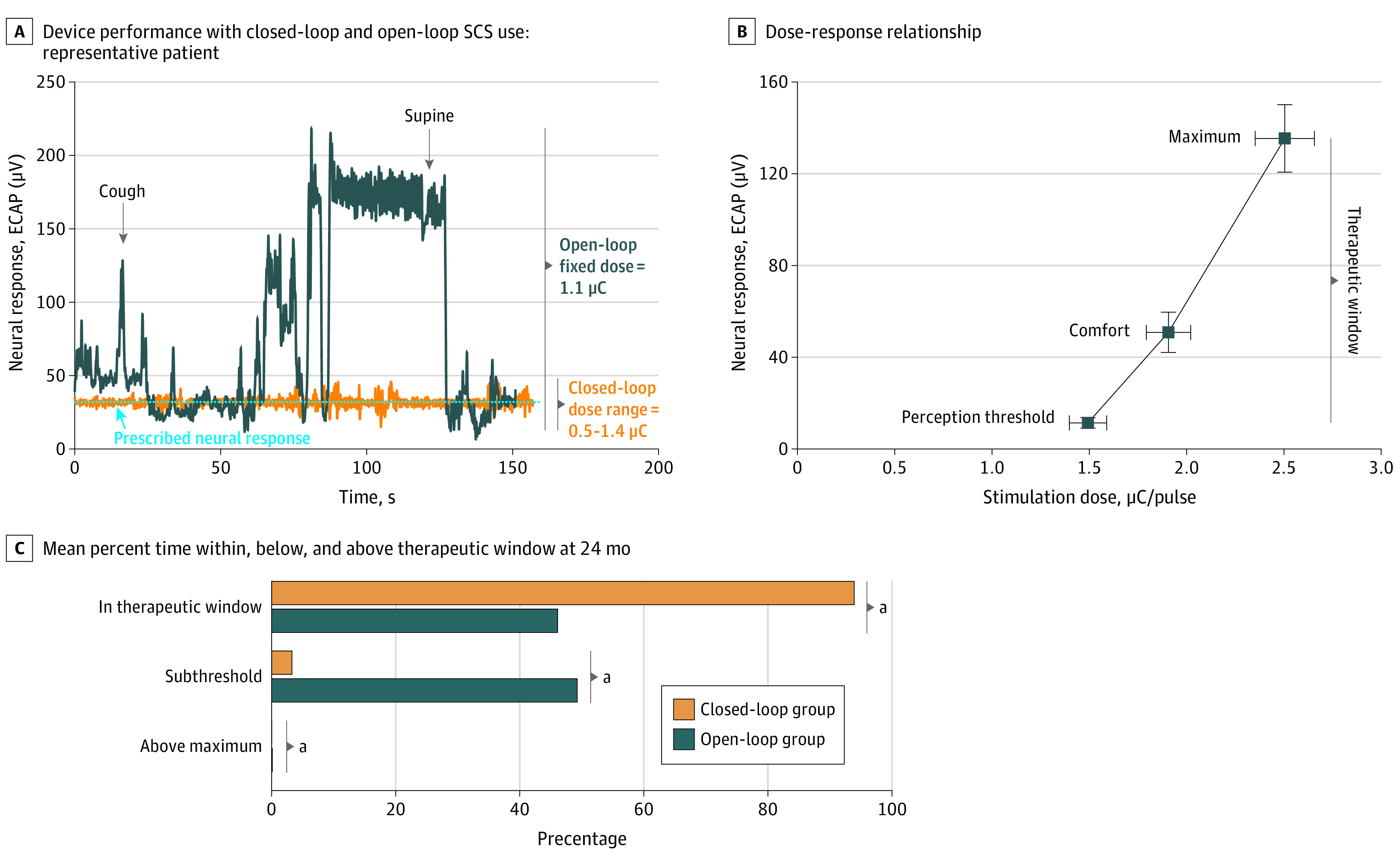
Importance: Chronic pain is debilitating and profoundly affects health-related quality of life. Spinal cord stimulation (SCS) is a well-established therapy for chronic pain; however, SCS has been limited by the inability to directly measure the elicited neural response, precluding confirmation of neural activation and continuous therapy. A novel SCS system measures the evoked compound action potentials (ECAPs) to produce a real-time physiological closed-loop control system.
Objective: To determine whether ECAP-controlled, closed-loop SCS is associated with better outcomes compared with fixed-output, open-loop SCS at 24 months following implant.
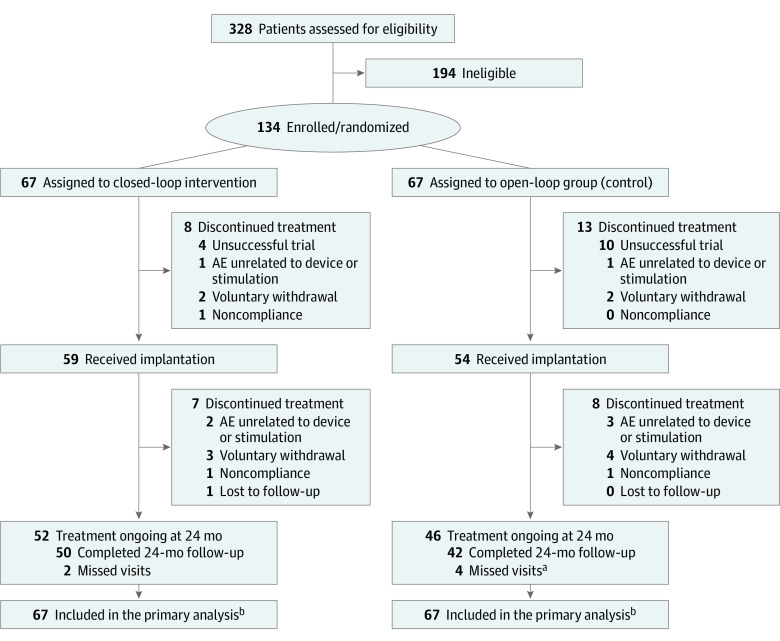
Design, setting, and participants: The Evoke study was a double-blind, randomized, controlled, parallel arm clinical trial with 36 months of follow-up. Participants were enrolled from February 2017 to 2018, and the study was conducted at 13 US investigation sites. SCS candidates with chronic, intractable back and leg pain refractory to conservative therapy, who consented, were screened. Key eligibility criteria included overall, back, and leg pain visual analog scale score of 60 mm or more; Oswestry Disability Index score of 41 to 80; stable pain medications; and no previous SCS. Analysis took place from October 2020 to April 2021.
Interventions: ECAP-controlled, closed-loop SCS was compared with fixed-output, open-loop SCS.
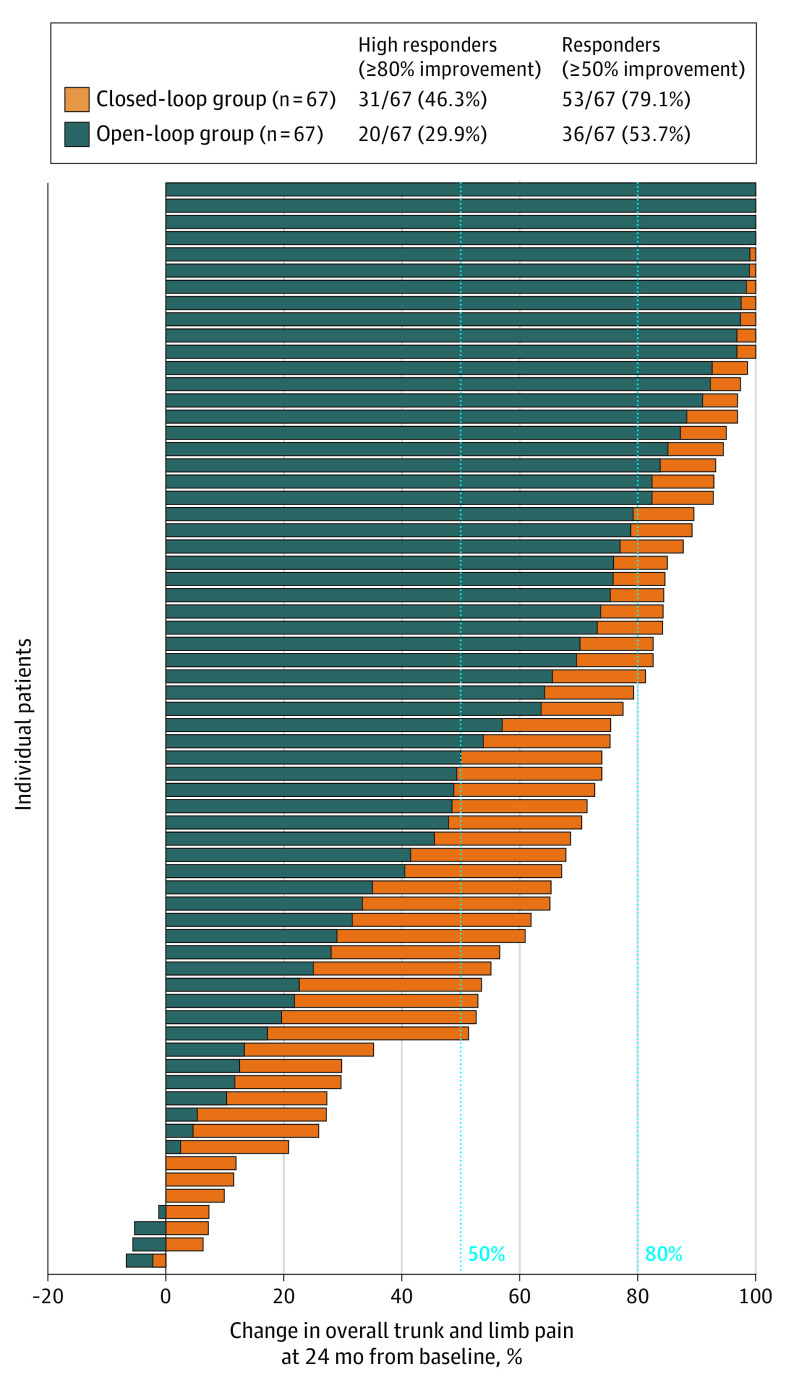
Main outcomes and measures: Reported here are the 24-month outcomes of the trial, which include all randomized patients in the primary and safety analyses. The primary outcome was a reduction of 50% or more in overall back and leg pain assessed at 3 and 12 months (previously published).
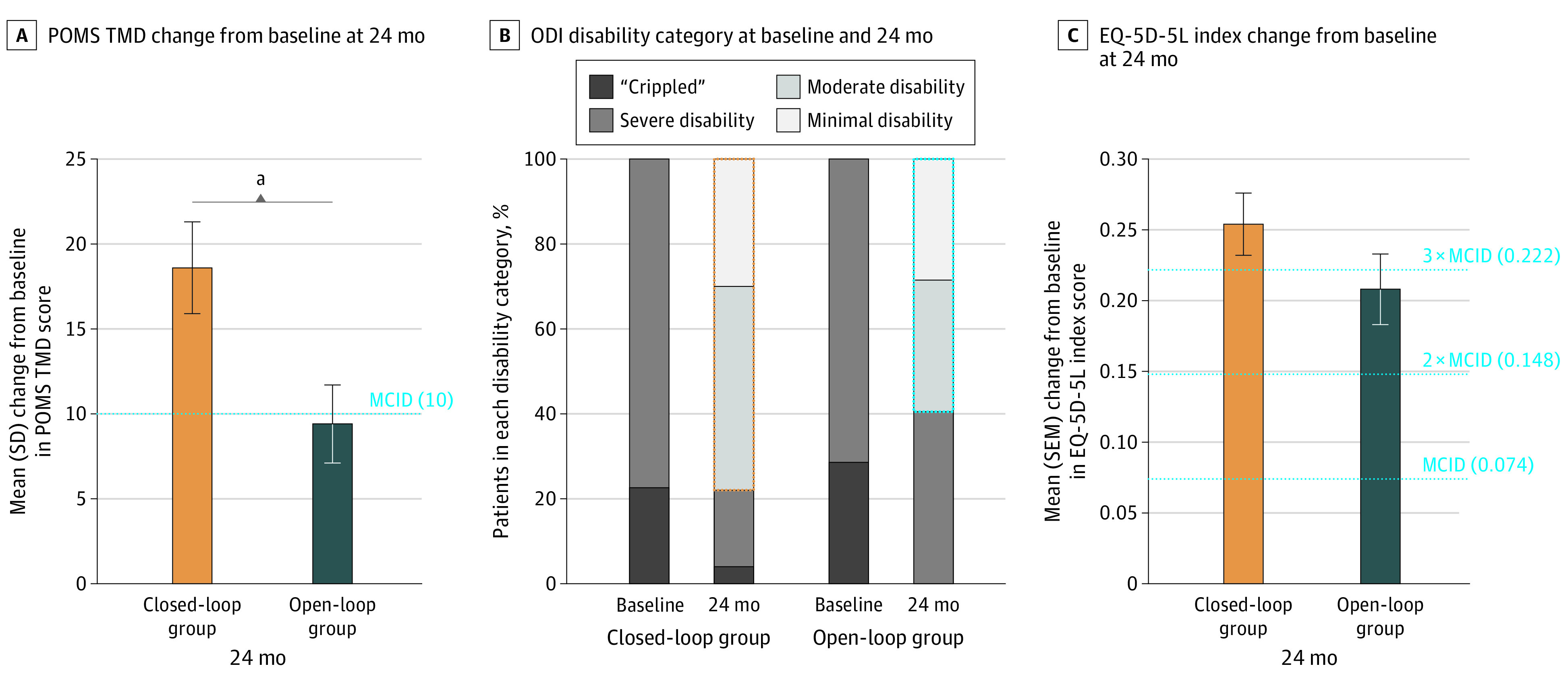
Results: Of 134 randomized patients, 65 (48.5%) were female and the mean (SD) age was 55.2 (10.6) years. At 24 months, significantly more closed-loop than open-loop patients were responders (≥50% reduction) in overall pain (53 of 67 [79.1%] in the closed-loop group; 36 of 67 [53.7%] in the open-loop group; difference, 25.4% [95% CI, 10.0%-40.8%]; P = .001). There was no difference in safety profiles between groups (difference in rate of study-related adverse events: 6.0 [95% CI, -7.8 to 19.7]). Improvements were also observed in health-related quality of life, physical and emotional functioning, and sleep, in parallel with opioid reduction or elimination. Objective neurophysiological measurements substantiated the clinical outcomes and provided evidence of activation of inhibitory pain mechanisms.
Conclusions and relevance: ECAP-controlled, closed-loop SCS, which elicited a more consistent neural response, was associated with sustained superior pain relief at 24 months, consistent with the 3- and 12-month outcomes.
Conflict of interest statement
Figures
References
-
- Katz N, Dworkin RH, North R, et al. . Research design considerations for randomized controlled trials of spinal cord stimulation for pain: initiative on methods, measurement, and pain assessment in clinical trials/Institute of Neuromodulation/International Neuromodulation Society recommendations. Pain. 2021;162(7):1935-1956. doi:10.1097/j.pain.0000000000002204 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
