

Impact of renal impairment on atrial fibrillation: ESC-EHRA EORP-AF Long-Term General Registry
- PMID: 35000206
- PMCID: PMC9287022
- DOI: 10.1111/eci.13745
Impact of renal impairment on atrial fibrillation: ESC-EHRA EORP-AF Long-Term General Registry
Abstract
Background: Atrial fibrillation (AF) and renal impairment share a bidirectional relationship with important pathophysiological interactions. We evaluated the impact of renal impairment in a contemporary cohort of patients with AF.
Methods: We utilised the ESC-EHRA EORP-AF Long-Term General Registry. Outcomes were analysed according to renal function by CKD-EPI equation. The primary endpoint was a composite of thromboembolism, major bleeding, acute coronary syndrome and all-cause death. Secondary endpoints were each of these separately including ischaemic stroke, haemorrhagic event, intracranial haemorrhage, cardiovascular death and hospital admission.
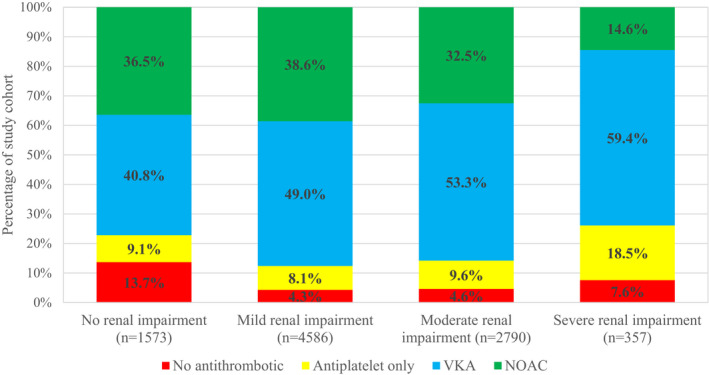
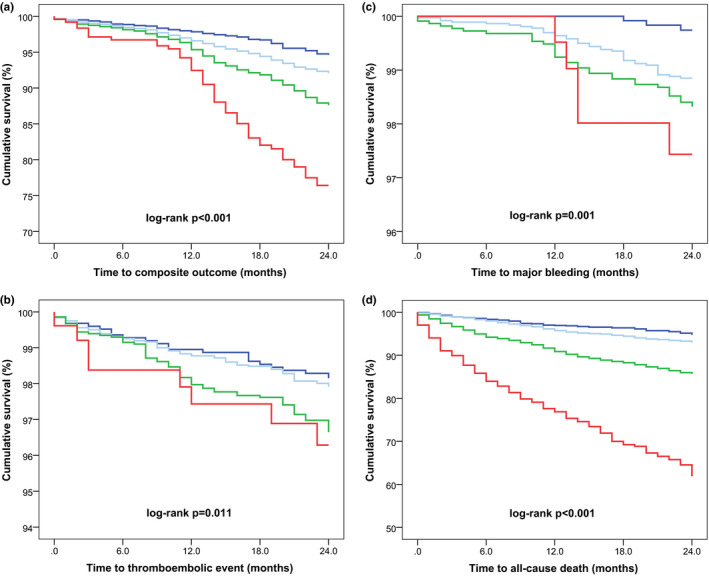
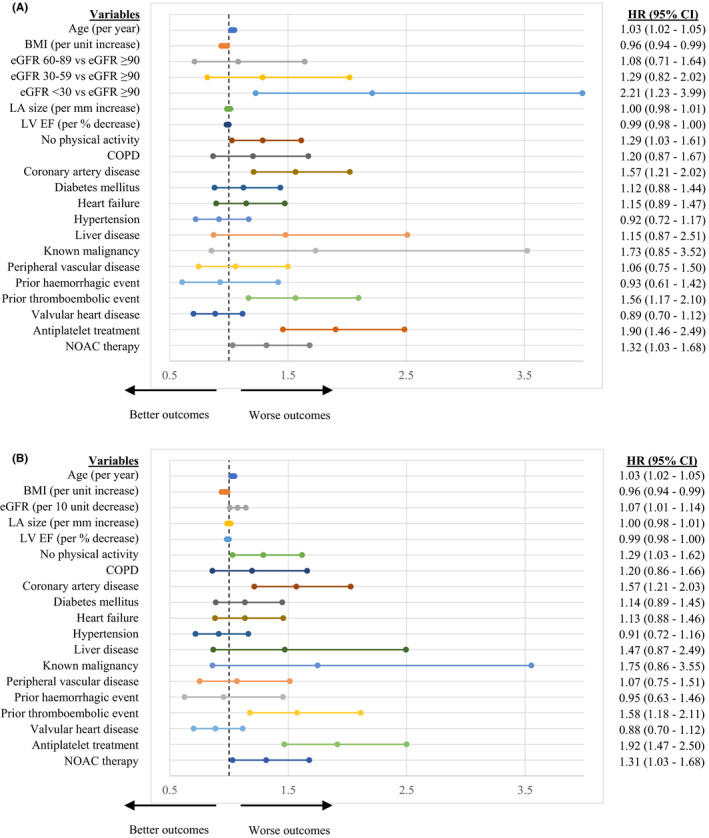
Results: A total of 9306 patients were included. The distribution of patients with no, mild, moderate and severe renal impairment at baseline were 16.9%, 49.3%, 30% and 3.8%, respectively. AF patients with impaired renal function were older, more likely to be females, had worse cardiac imaging parameters and multiple comorbidities. Among patients with an indication for anticoagulation, prescription of these agents was reduced in those with severe renal impairment, p < .001. Over 24 months, impaired renal function was associated with significantly greater incidence of the primary composite outcome and all secondary outcomes. Multivariable Cox regression analysis demonstrated an inverse relationship between eGFR and the primary outcome (HR 1.07 [95% CI, 1.01-1.14] per 10 ml/min/1.73 m2 decrease), that was most notable in patients with eGFR <30 ml/min/1.73 m2 (HR 2.21 [95% CI, 1.23-3.99] compared to eGFR ≥90 ml/min/1.73 m2 ).
Conclusion: A significant proportion of patients with AF suffer from concomitant renal impairment which impacts their overall management. Furthermore, renal impairment is an independent predictor of major adverse events including thromboembolism, major bleeding, acute coronary syndrome and all-cause death in patients with AF.
Keywords: atrial fibrillation; chronic kidney disease; death; kidney failure; major bleeding; outcome; thromboembolism.
© 2022 The Authors. European Journal of Clinical Investigation published by John Wiley & Sons Ltd on behalf of Stichting European Society for Clinical Investigation Journal Foundation.
Conflict of interest statement
GB: small speaker's fees from Medtronic, Boston, Biotronik, Boehringer and Bayer, outside of the submitted work. FM: receiving grants from Ferrer, and personal fees from Bayer, Pfizer/BMS. Boehringer‐Ingelheim and Astra‐Zeneca outside the submitted work. CBL: receiving grants from Medtronic, Cardiome and personal fees from Bayer, Sanofi, Boston Scientific and Merck Sharp & Dohme outside the submitted work. TSP: Consultant for Bayer and Pfizer, no fees. LF: consultant or speaker fees of small amounts for Bayer, BMS/Pfizer, Boehringer Ingelheim, Medtronic and Novartis outside of this work. GYHL: Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim and Daiichi‐Sankyo. No fees are received personally. Other authors declare no conflict of interest.
Figures
References
-
- KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1‐150. - PubMed
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038‐2047. - PubMed
-
- Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch Intern Med. 1995;155(5):469‐473. - PubMed
-
- Ding WY, Gupta D, Wong CF, Lip GYH. Pathophysiology of atrial fibrillation and chronic kidney disease. Cardiovasc Res. 2021;117(4):1046‐1059. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
