

The Individual Ictal Fingerprint: Combining Movement Measures With Ultra Long-Term Subcutaneous EEG in People With Epilepsy
- PMID: 35002910
- PMCID: PMC8733463
- DOI: 10.3389/fneur.2021.718329
The Individual Ictal Fingerprint: Combining Movement Measures With Ultra Long-Term Subcutaneous EEG in People With Epilepsy
Abstract
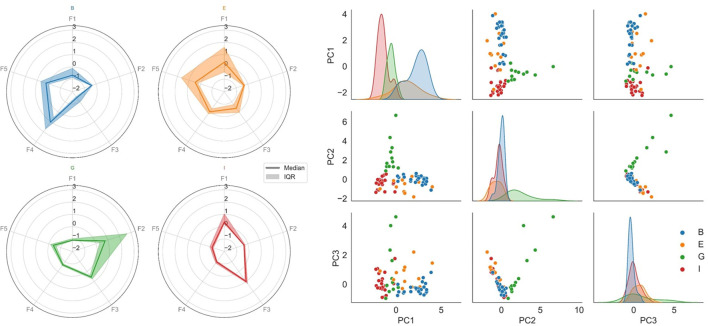
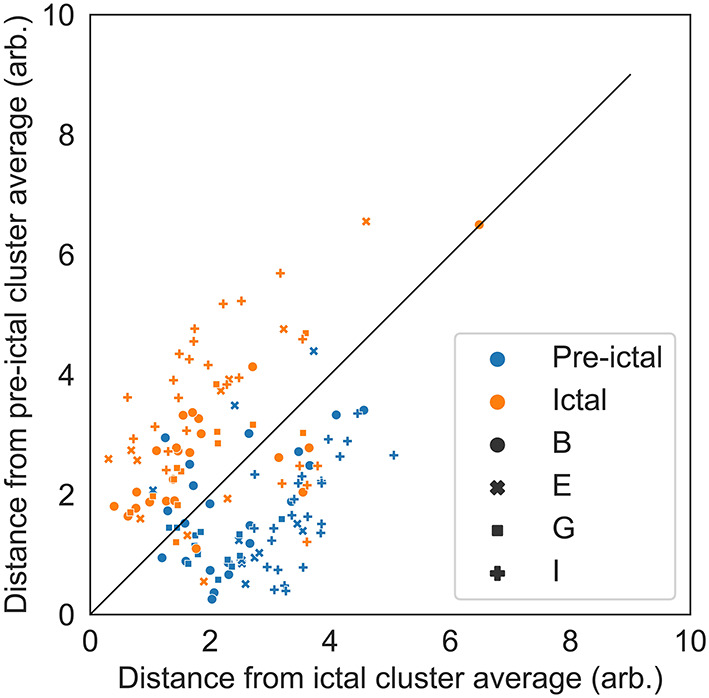
Background: Epileptic seizures are caused by abnormal brain wave hypersynchronization leading to a range of signs and symptoms. Tools for detecting seizures in everyday life typically focus on cardiac rhythm, electrodermal activity, or movement (EMG, accelerometry); however, these modalities are not very effective for non-motor seizures. Ultra long-term subcutaneous EEG-devices can detect the electrographic changes that do not depend on clinical changes. Nonetheless, this also means that it is not possible to assess whether a seizure is clinical or subclinical based on an EEG signal alone. Therefore, we combine EEG and movement-related modalities in this work. We focus on whether it is possible to define an individual "multimodal ictal fingerprint" which can be exploited in different epilepsy management purposes. Methods: This study used ultra long-term data from an outpatient monitoring trial of persons with temporal lobe epilepsy obtained with a subcutaneous EEG recording system. Subcutaneous EEG, an EMG estimate and chest-mounted accelerometry were extracted from four persons showing more than 10 well-defined electrographic seizures each. Numerous features were computed from all three modalities. Based on these, the Gini impurity measure of a Random Forest classifier was used to select the most discriminative features for the ictal fingerprint. A total of 74 electrographic seizures were analyzed. Results: The optimal individual ictal fingerprints included features extracted from all three tested modalities: an acceleration component; the power of the estimated EMG activity; and the relative power in the delta (0.5-4 Hz), low theta (4-6 Hz), and high theta (6-8 Hz) bands of the subcutaneous EEG. Multimodal ictal fingerprints were established for all persons, clustering seizures within persons, while separating seizures across persons. Conclusion: The existence of multimodal ictal fingerprints illustrates the benefits of combining multiple modalities such as EEG, EMG, and accelerometry in future epilepsy management. Multimodal ictal fingerprints could be used by doctors to get a better understanding of the individual seizure semiology of people with epilepsy. Furthermore, the multimodal ictal fingerprint gives a better understanding of how seizures manifest simultaneously in different modalities. A knowledge that could be used to improve seizure acknowledgment when reviewing EEG without video.
Keywords: EMG; accelerometry; epilepsy; ictal fingerprint; seizure detection; subcutaneous EEG.
Copyright © 2021 Kjaer, Remvig, Helge and Duun-Henriksen.
Conflict of interest statement
TK consults for UNEEG medical A/S. LR, AH, and JDH are employees of UNEEG medical A/S.
Figures

References
LinkOut - more resources
Full Text Sources
Medical