

Urinary Soluble CD163 Levels Predict IgA Nephropathy Remission Status
- PMID: 35003086
- PMCID: PMC8733336
- DOI: 10.3389/fimmu.2021.769802
Urinary Soluble CD163 Levels Predict IgA Nephropathy Remission Status
Abstract
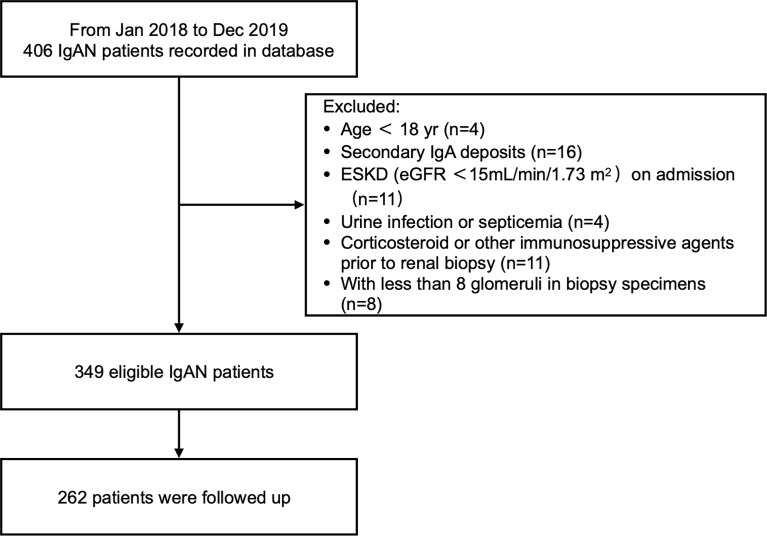
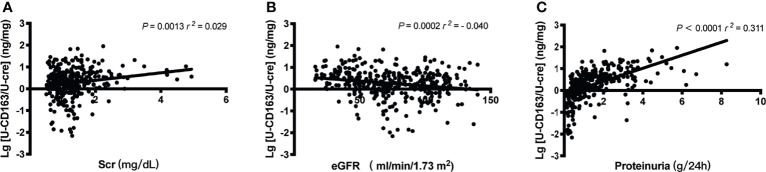
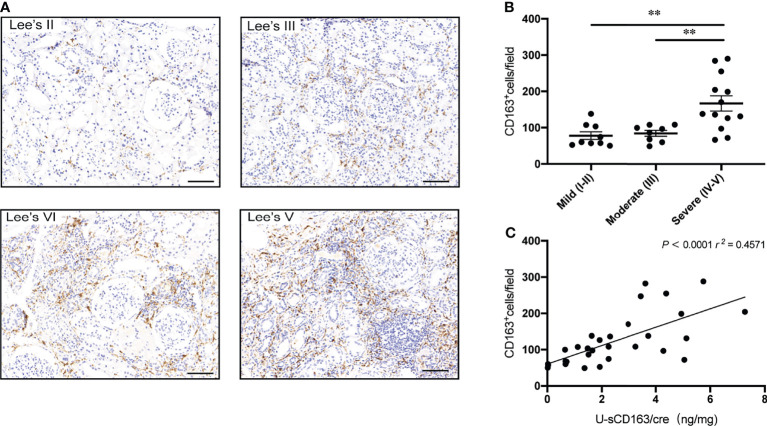
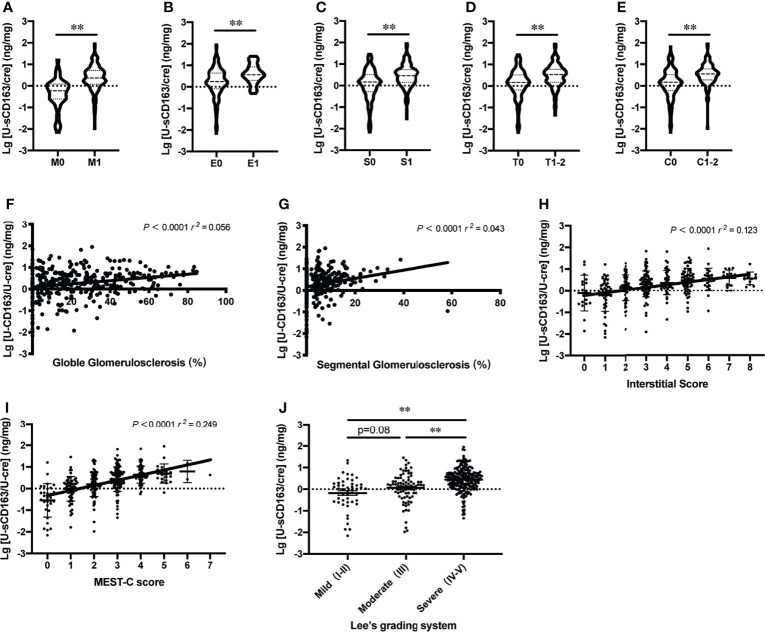
Noninvasive biomarkers of disease activity are needed to predict disease remission status in patients with IgA nephropathy (IgAN). Soluble CD163 (sCD163), shed by monocytes and macrophages, is a potential biomarker in diseases associated with excessive macrophage activation. We investigated the association of urinary sCD163 (u-sCD163) with histopathological activity and clinical manifestations in 349 patients with biopsy-diagnosed IgAN. U-sCD163 was measured via enzyme-linked immunosorbent assay. In patients with IgAN, higher u-sCD163 levels were associated with histological lesions of greater severity, as well as more proteinuria and poorer renal function. Additionally, u-sCD163 was correlated with infiltration of tubulointerstitial CD163+ macrophages. High u-sCD163 levels (>3.57 ng/mg Cr) were associated with a 2.66-fold greater risk for IgAN remission failure in adjusted analyses. Adding u-sCD163 levels to the model containing clinical data at biopsy and MEST-C score significantly improved the risk prediction of IgAN remission status (AUC 0.788). Together, our results suggest that u-sCD163 may be a useful noninvasive biomarker to evaluate disease severity and remission status of IgAN.
Keywords: IgA nephropathy; biomarker; macrophages; remission status; urinary soluble CD163.
Copyright © 2021 Gong, Jin, Li, Jiang, Zhang, Shen, Wang, Zhou, Liu, Xu, Ding, Shi and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Urinary Soluble CD163 in Active Renal Vasculitis.J Am Soc Nephrol. 2016 Sep;27(9):2906-16. doi: 10.1681/ASN.2015050511. Epub 2016 Mar 3. J Am Soc Nephrol. 2016. PMID: 26940094 Free PMC article.
-
Urinary soluble CD163 level reflects glomerular inflammation in human lupus nephritis.Nephrol Dial Transplant. 2016 Dec;31(12):2023-2033. doi: 10.1093/ndt/gfw214. Epub 2016 May 30. Nephrol Dial Transplant. 2016. PMID: 27242373
-
Correlation of Urinary Soluble CD163 Levels With Disease Activity and Treatment Response in IgA Nephropathy.Kidney Int Rep. 2024 Aug 3;9(10):3016-3026. doi: 10.1016/j.ekir.2024.07.031. eCollection 2024 Oct. Kidney Int Rep. 2024. PMID: 39430181 Free PMC article.
-
Elevated Numbers of Circulating Very Small Embryonic-Like Stem Cells (VSELs) and Intermediate CD14++CD16+ Monocytes in IgA Nephropathy.Stem Cell Rev Rep. 2018 Oct;14(5):686-693. doi: 10.1007/s12015-018-9840-y. Stem Cell Rev Rep. 2018. PMID: 30022351 Free PMC article. Review.
-
Soluble CD163.Scand J Clin Lab Invest. 2012 Feb;72(1):1-13. doi: 10.3109/00365513.2011.626868. Epub 2011 Nov 7. Scand J Clin Lab Invest. 2012. PMID: 22060747 Review.
Cited by
-
A Histology-Guided Approach to the Management of Patients with Lupus Nephritis: Are We There Yet?Biomedicines. 2022 Jun 15;10(6):1409. doi: 10.3390/biomedicines10061409. Biomedicines. 2022. PMID: 35740431 Free PMC article. Review.
-
Mizoribine halts kidney fibrosis in childhood IgA nephropathy: association with modulation of M2-type macrophages.Pediatr Nephrol. 2023 Jun;38(6):1831-1842. doi: 10.1007/s00467-022-05786-w. Epub 2022 Nov 10. Pediatr Nephrol. 2023. PMID: 36357635
-
Pharmacovigilance in Cell and Gene Therapy: Evolving Challenges in Risk Management and Long-Term Follow-Up.Drug Saf. 2025 Aug 9. doi: 10.1007/s40264-025-01596-9. Online ahead of print. Drug Saf. 2025. PMID: 40783602 Review.
-
CD163 detection in immune check-point inhibitors-related acute interstitial nephritis.Clin Kidney J. 2025 Feb 18;18(3):sfaf009. doi: 10.1093/ckj/sfaf009. eCollection 2025 Mar. Clin Kidney J. 2025. PMID: 40052170 Free PMC article.
-
Urinary N-Acetyl-Beta-D-Glucosaminidase levels predict immunoglobulin a nephropathy remission status.BMC Nephrol. 2023 Jul 14;24(1):208. doi: 10.1186/s12882-023-03262-7. BMC Nephrol. 2023. PMID: 37452282 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous