

Correlation between Renal Artery Anatomy and Hypertension: A Retrospective Analysis of 3000 Patients
- PMID: 35003315
- PMCID: PMC8731270
- DOI: 10.1155/2021/9957361
Correlation between Renal Artery Anatomy and Hypertension: A Retrospective Analysis of 3000 Patients
Abstract
Objective: To assess the correlation between renal artery anatomy and blood pressure in Undiagnosed Hypertension and Diagnosed Hypertension.
Methods: The renal artery CT scanning imaging data and laboratory data of 3000 inpatients and outpatients were collected retrospectively in 4 centers of China. Morphometric parameters were assessed using the quantitative vascular analysis (unit: mM).
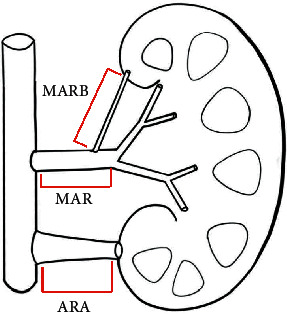
Results: 687 cases (23.2%) had accessory renal arteries unilaterally, and 216 cases (7.3%) had bilateral accessory renal arteries, including left kidney 825 (27.9%) and right kidney 798 (27.0%). The presence of accessory renal arteries and renal artery branches was higher in the diagnosed hypertension group as compared with the undiagnosed hypertension group (MARB, pp < 0.001; ARA, p < 0.001; others, p < 0.001). Consequently, multivariate regression analysis showed that age (OR = 2.519 (95% CI: 0.990-6.411, p < 0.001)), dyslipidemia (OR = 1.187 (95% CI: 0.960-1.454, p = 0.007)), renal hilum Outside the main renal artery branch (MRAB) (OR = 2.069 (95% CI: 1.614-2.524, p = 0.002)), and accessory renal artery (ARA) (OR = 2.071 (95% CI: 1.614-2.634, p = 0.001)) were risk factors of hypertension. In addition, higher renin activity was associated with ARA patients (2.19 ± 2.91 vs. 1.75 ± 2.85, p < 0.001).
Conclusions: When comparing renal arteries side by side, the anatomical length of the renal arteries is significantly different. In addition, the prevalence of accessory renal arteries and renal artery branches is higher in the hypertension group. The auxiliary renal artery and the main renal artery branch outside the renal portal are independent factors of hypertension. Renal sympathetic nerve activity is affected by renin activity and is related to the accessory renal artery.
Copyright © 2021 Jiayi Shen et al.
Conflict of interest statement
The authors declare there are no conflicts of interest.
Figures



Similar articles
-
Anatomical and procedural determinants of ambulatory blood pressure lowering following catheter-based renal denervation using radiofrequency.Cardiovasc Revasc Med. 2018 Oct-Nov;19(7 Pt B):845-851. doi: 10.1016/j.carrev.2018.02.016. Epub 2018 Mar 2. Cardiovasc Revasc Med. 2018. PMID: 29555535 Free PMC article. Clinical Trial.
-
Relationship between accessory renal arteries and resistant hypertension: A cohort study.J Med Vasc. 2023 Feb;48(1):18-23. doi: 10.1016/j.jdmv.2023.03.001. Epub 2023 Apr 5. J Med Vasc. 2023. PMID: 37120265
-
Persistent Increase in Blood Pressure After Renal Nerve Stimulation in Accessory Renal Arteries After Sympathetic Renal Denervation.Hypertension. 2016 Jun;67(6):1211-7. doi: 10.1161/HYPERTENSIONAHA.115.06604. Epub 2016 Apr 25. Hypertension. 2016. PMID: 27113046
-
Clinical effect of accessory renal artery coverage after endovascular repair of aneurysms in abdominal and thoracoabdominal aorta.J Vasc Surg. 2021 Dec;74(6):2104-2113.e7. doi: 10.1016/j.jvs.2021.06.032. Epub 2021 Jun 29. J Vasc Surg. 2021. PMID: 34197943
-
Variations in branching pattern of renal artery and arrangement of hilar structures in the left kidney: clinical correlations, a case report.Ital J Anat Embryol. 2012;117(2):118-22. Ital J Anat Embryol. 2012. PMID: 23420999 Review.
Cited by
-
The accessory renal arteries: A systematic review with meta-analysis.Clin Anat. 2025 Sep;38(6):660-672. doi: 10.1002/ca.24255. Epub 2024 Dec 8. Clin Anat. 2025. PMID: 39648312 Free PMC article. Review.
-
Multiple Treatment Strategies of Accessory Renal Artery Related Hypertension: Report of Two Cases and Literature Review.J Clin Hypertens (Greenwich). 2024 Dec;26(12):1449-1456. doi: 10.1111/jch.14916. Epub 2024 Nov 15. J Clin Hypertens (Greenwich). 2024. PMID: 39545713 Free PMC article. Review.
-
Effect of Accessory Renal Arteries on Essential Hypertension and Related Mechanisms.J Am Heart Assoc. 2024 Feb 20;13(4):e030427. doi: 10.1161/JAHA.123.030427. Epub 2024 Feb 13. J Am Heart Assoc. 2024. PMID: 38348775 Free PMC article.
-
Primary Aldosteronism Masked by Accessory Renal Arteries: A Case Report.J Clin Med. 2022 Oct 25;11(21):6276. doi: 10.3390/jcm11216276. J Clin Med. 2022. PMID: 36362504 Free PMC article.
-
Accessory renal arteries - a source of hypertension: A case report.World J Clin Cases. 2023 Mar 6;11(7):1506-1512. doi: 10.12998/wjcc.v11.i7.1506. World J Clin Cases. 2023. PMID: 36926389 Free PMC article.
References
-
- Zeller T. Renal artery stenosis--new insights and developments. Deutsche Medizinische Wochenschrift (1946) . 2015;140:184–187. - PubMed
-
- Aboyans V., Desormais I., Magne J., Morange G., Mohty D., Lacroix P. Renal artery stenosis in patients with peripheral artery disease: prevalence, risk factors and long-term prognosis. European Journal of Vascular and Endovascular Surgery . 2017;53(3):380–385. doi: 10.1016/j.ejvs.2016.10.029. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
