

Residual Acetabular Dysplasia in the Reduced Hip
- PMID: 35003538
- PMCID: PMC8688620
- DOI: 10.1007/s43465-021-00515-1
Residual Acetabular Dysplasia in the Reduced Hip
Abstract
Background: Residual acetabular dysplasia occurs in up to a third of patients treated successfully for developmental dysplasia of the hip (DDH) and has been found to be a significant risk factor for early hip osteoarthritis (OA).
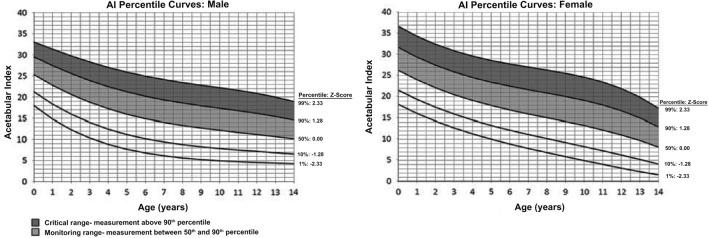
Discussion: Age at the time of initial reduction and the initial severity of DDH have been linked to residual acetabular dysplasia. An anteroposterior pelvic radiograph is the main diagnostic modality, but MRI also provides valuable information, particularly in equivocal cases. The literature supports intervening when significant residual acetabular dysplasia persists at 4-5 years of age, and common surgical indications include acetabular index (AI) > 25°-30°, lateral center-edge angle (LCEA) < 8°-10°, and a broken Shenton's line on radiographs; and a cartilaginous acetabular angle (CAI) > 18°, cartilaginous center-edge angle (CCE) < 13°, and/or the presence of high-signal intensity areas on MRI. Surgical options include redirectional pelvic osteotomies and reshaping acetabuloplasties, which provide comparable radiographic and clinical results.
Conclusion: RAD is common after treatment of DDH and requires regular follow-up for diagnosis and appropriate management to decrease the long-term risk of OA. Long-term outcomes of patients treated with pelvic osteotomies are generally favorable, and the risk of OA can be decreased, although the risk of total hip replacement in the long-term remains.
Keywords: Developmental dysplasia of the hip; Osteoarthritis; Pediatric hip; Pediatrics; Pelvic osteotomy; Residual acetabular dysplasia.
© Indian Orthopaedics Association 2021.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures




References
-
- Clohisy JC, Beaulé PE, O'Malley A, et al. Aoa symposium: hip disease in the young adult—current concepts of etiology and surgical treatment. Journal of Bone and Joint Surgery. 2008;90(10):2267–2281. - PubMed
-
- Weinstein SL. Natural history of congenital hip dislocation (cdh) and hip dysplasia. Clinical Orthopaedics and Related Research. 1987;225:62–76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials