

Interventions to reduce preterm birth and stillbirth, and improve outcomes for babies born preterm in low- and middle-income countries: A systematic review
- PMID: 35003711
- PMCID: PMC8709903
- DOI: 10.7189/jogh.11.04050
Interventions to reduce preterm birth and stillbirth, and improve outcomes for babies born preterm in low- and middle-income countries: A systematic review
Abstract
Background: Reducing preterm birth and stillbirth and improving outcomes for babies born too soon is essential to reduce under-5 mortality globally. In the context of a rapidly evolving evidence base and problems with extrapolating efficacy data from high- to low-income settings, an assessment of the evidence for maternal and newborn interventions specific to low- and middle-income countries (LMICs) is required.
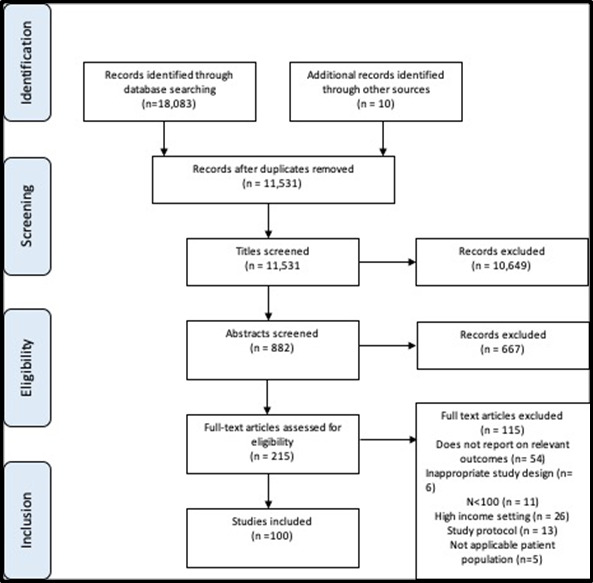
Methods: A systematic review of the literature was done. We included all studies performed in LMICs since the Every Newborn Action Plan, between 2013 - 2018, which reported on interventions where the outcome assessed was reduction in preterm birth or stillbirth incidence and/or a reduction in preterm infant neonatal mortality. Evidence was categorised according to maternal or neonatal intervention groups and a narrative synthesis conducted.
Results: 179 studies (147 primary evidence studies and 32 systematic reviews) were identified in 82 LMICs. 81 studies reported on maternal interventions and 98 reported on neonatal interventions. Interventions in pregnant mothers which resulted in significant reductions in preterm birth and stillbirth were (i) multiple micronutrient supplementation and (ii) enhanced quality of antenatal care. Routine antenatal ultrasound in LMICs increased identification of fetal antenatal conditions but did not reduce stillbirth or preterm birth due to the absence of services to manage these diagnoses. Interventions in pre-term neonates which improved their survival included (i) feeding support including probiotics and (ii) thermal regulation. Improved provision of neonatal resuscitation did not improve pre-term mortality rates, highlighting the importance of post-resuscitation care. Community mobilisation, for example through community education packages, was found to be an effective way of delivering interventions.
Conclusions: Evidence supports the implementation of several low-cost interventions with the potential to deliver reductions in preterm birth and stillbirth and improve outcomes for preterm babies in LMICs. These, however, must be complemented by overall health systems strengthening to be effective. Quality improvement methodology and learning health systems approaches can provide important means of understanding and tackling implementation challenges within local contexts. Further pragmatic efficacy trials of interventions in LMICs are essential, particularly for interventions not previously tested in these contexts.
Copyright © 2021 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Competing interests: The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author), and declare no conflicts of interest.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
