

Nomograms Combining Ultrasonic Features With Clinical and Pathological Features for Estimation of Delphian Lymph Node Metastasis Risk in Papillary Thyroid Carcinoma
- PMID: 35004316
- PMCID: PMC8733604
- DOI: 10.3389/fonc.2021.792347
Nomograms Combining Ultrasonic Features With Clinical and Pathological Features for Estimation of Delphian Lymph Node Metastasis Risk in Papillary Thyroid Carcinoma
Abstract
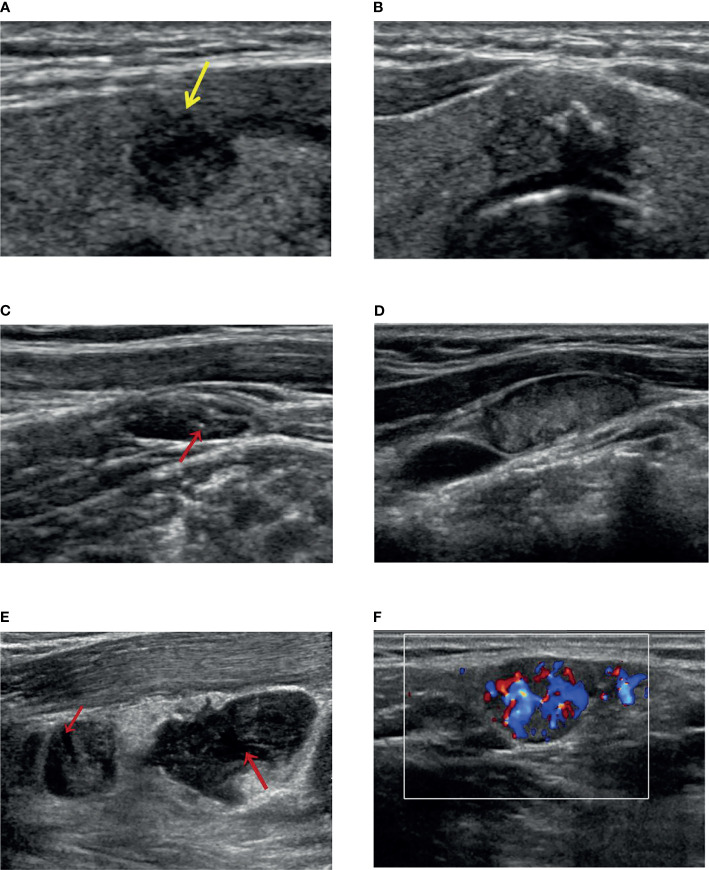
Background: This work explores the clinical significance of Delphian lymph nodes (DLN) in thyroid papillary carcinoma (PTC). At the same time, a nomogram is constructed based on clinical, pathological, and ultrasonic (US) features to evaluate the possibility of DLN metastasis (DLNM) in PTC patients. This is the first study to predict DLNM using US characteristics.
Methods: A total of 485 patients, surgically diagnosed with PTC between February 2017 and June 2021, all of whom underwent thyroidectomy, were included in the study. Using the clinical, pathological, and US information of patients, the related factors of DLNM were retrospectively analyzed. The risk factors associated with DLNM were identified through univariate and multivariate analyses. According to clinical + pathology, clinical + US, and clinical + US + pathology, the predictive nomogram for DLNM was established and validated.
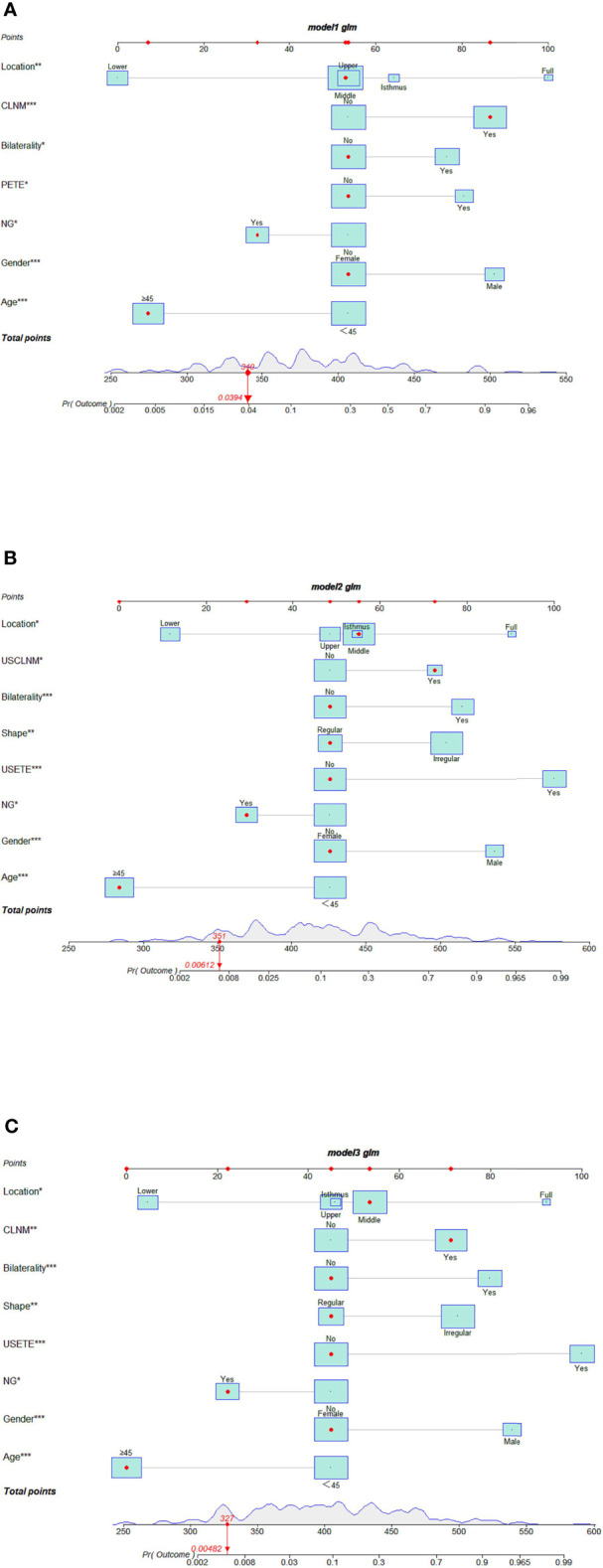
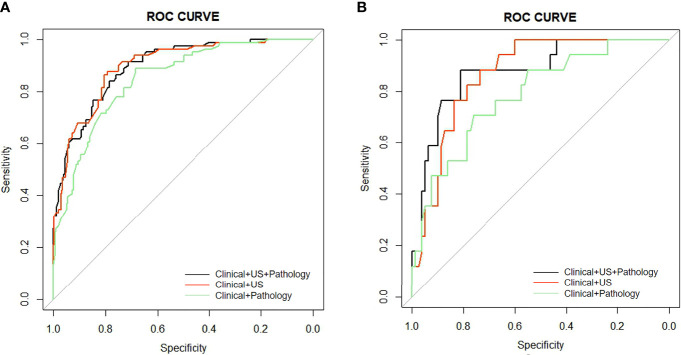
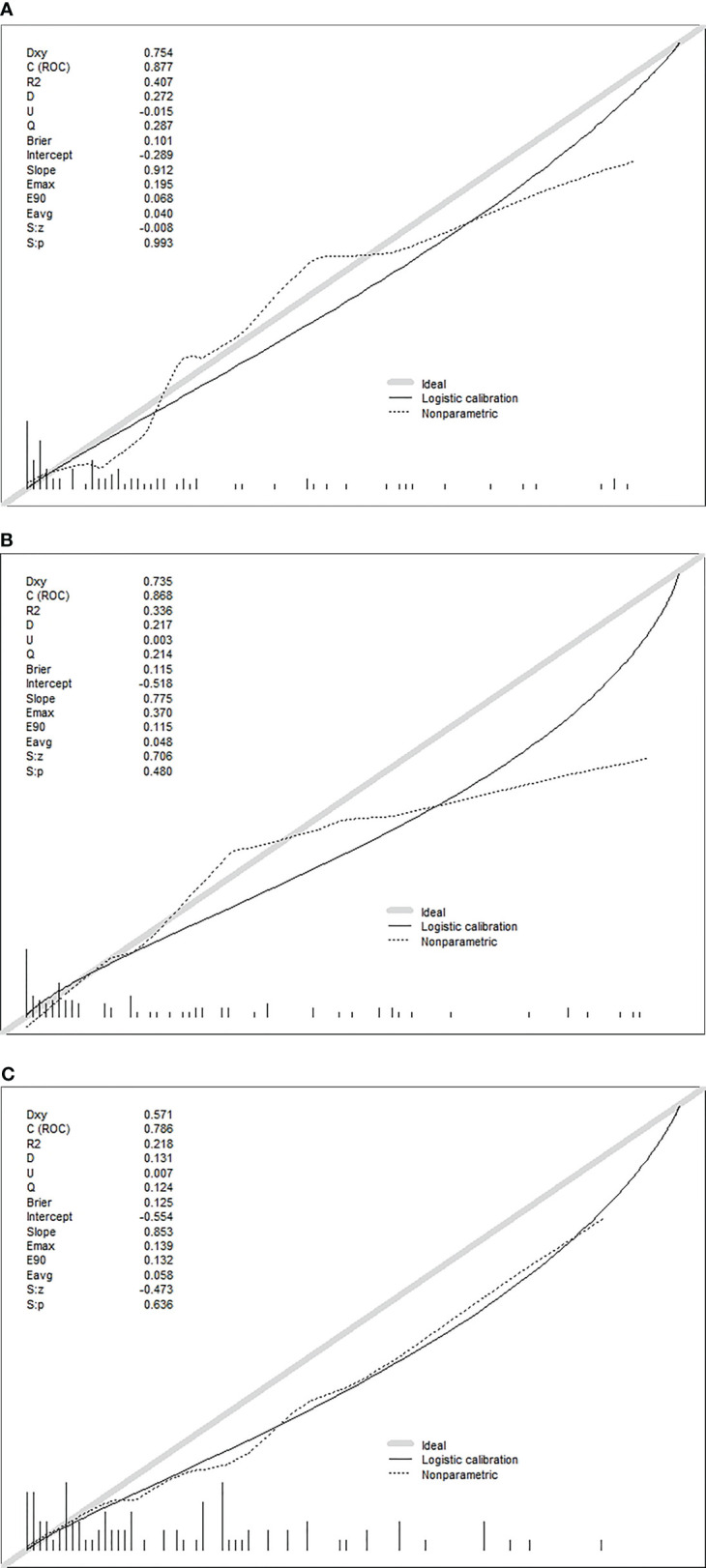
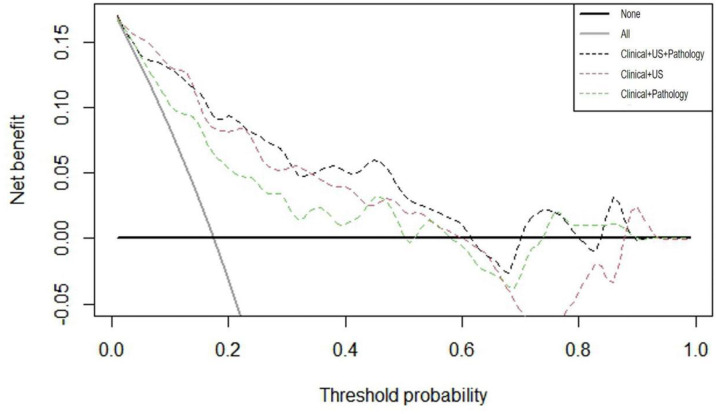
Results: Of the 485 patients with DLN, 98 (20.2%) exhibited DLNM. The DLNM positive group had higher positive rates of central lymph node metastasis (CLNM), lateral lymph node metastasis (LLNM), and T3b-T4b thyroid tumors than the negative rates. The number of CLNM and LLNM lymph nodes in the DLNM+ group was higher as compared to that in the DLNM- group. Multivariate analysis demonstrated that the common independent risk factors of the three prediction models were male, bilaterality, and located in the isthmus. Age ≥45 years, located in the lower pole, and nodural goiter were protective factors. In addition, the independent risk factors were classified as follows: (I) P-extrathyroidal extension (ETE) and CLNM based on clinical + pathological characteristics; (II) US-ETE and US-CLNM based on clinical + US characteristics; and (III) US-ETE and CLNM based on clinical +US + pathological features. Better diagnostic efficacy was reported with clinical + pathology + US diagnostic model than that of clinical + pathology diagnostic model (AUC 0.872 vs. 0.821, p = 0.039). However, there was no significant difference between clinical + pathology + US diagnostic model and clinical + US diagnostic model (AUC 0.872 vs. 0.821, p = 0.724).
Conclusions: This study found that DLNM may be a sign that PTC is more invasive and has extensive lymph node metastasis. By exploring the clinical, pathology, and US characteristics of PTC progression to DLNM, three prediction nomograms, established according to different combinations of features, can be used in different situations to evaluate the transfer risk of DLN.
Keywords: Delphian lymph nodes metastasis; nomograms; papillary thyroid carcinoma; risk factors; ultrasound.
Copyright © 2021 Qi, Xu, Zhang, Guo, Huang, Chen, Li and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Meta-analysis of the effect and clinical significance of Delphian lymph node metastasis in papillary thyroid cancer.Front Endocrinol (Lausanne). 2024 Jan 19;14:1295548. doi: 10.3389/fendo.2023.1295548. eCollection 2023. Front Endocrinol (Lausanne). 2024. PMID: 38313842 Free PMC article.
-
Predictive value of the Delphian lymph node in cervical lymph node metastasis of papillary thyroid carcinoma.Eur J Surg Oncol. 2021 Jul;47(7):1727-1733. doi: 10.1016/j.ejso.2021.02.010. Epub 2021 Feb 18. Eur J Surg Oncol. 2021. PMID: 33632590
-
Significance and Predictive Value of Delphian Lymph Node in Papillary Thyroid Carcinoma.Curr Med Imaging. 2025;21:e15734056360214. doi: 10.2174/0115734056360214250215155608. Curr Med Imaging. 2025. PMID: 40143394
-
Analysis of the Clinical Value of Delphian Lymph Node Metastasis in Papillary Thyroid Carcinoma.J Oncol. 2022 Jun 10;2022:8108256. doi: 10.1155/2022/8108256. eCollection 2022. J Oncol. 2022. PMID: 35720222 Free PMC article.
-
Shear wave elastography combined with gray-scale ultrasound for predicting central lymph node metastasis of papillary thyroid carcinoma.Surg Oncol. 2021 Mar;36:1-6. doi: 10.1016/j.suronc.2020.11.004. Epub 2020 Nov 25. Surg Oncol. 2021. PMID: 33271464 Review.
Cited by
-
Nomogram for preoperative estimation risk of cervical lymph node metastasis in medullary thyroid carcinoma.Front Oncol. 2022 Oct 12;12:883429. doi: 10.3389/fonc.2022.883429. eCollection 2022. Front Oncol. 2022. PMID: 36313643 Free PMC article.
-
Prelaryngeal and/or pretracheal lymph node metastasis could help to identify papillary thyroid carcinoma with intermediate risk from unilateral lobe cT1-2N0 papillary thyroid carcinoma.Front Endocrinol (Lausanne). 2023 Apr 14;14:1156664. doi: 10.3389/fendo.2023.1156664. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37124749 Free PMC article.
-
A machine learning model utilizing Delphian lymph node characteristics to predict contralateral central lymph node metastasis in papillary thyroid carcinoma: a prospective multicenter study.Int J Surg. 2025 Jan 1;111(1):360-370. doi: 10.1097/JS9.0000000000002020. Int J Surg. 2025. PMID: 39110573 Free PMC article.
-
Meta-analysis of the effect and clinical significance of Delphian lymph node metastasis in papillary thyroid cancer.Front Endocrinol (Lausanne). 2024 Jan 19;14:1295548. doi: 10.3389/fendo.2023.1295548. eCollection 2023. Front Endocrinol (Lausanne). 2024. PMID: 38313842 Free PMC article.
-
Accuracy of papillary thyroid cancer prognostic nomograms: a systematic review.Endocr Connect. 2023 Mar 10;12(4):e220457. doi: 10.1530/EC-22-0457. Print 2023 Apr 1. Endocr Connect. 2023. PMID: 36662681 Free PMC article.
References
LinkOut - more resources
Full Text Sources