

Tackling the Challenges of Graft Healing After Anterior Cruciate Ligament Reconstruction-Thinking From the Endpoint
- PMID: 35004636
- PMCID: PMC8727521
- DOI: 10.3389/fbioe.2021.756930
Tackling the Challenges of Graft Healing After Anterior Cruciate Ligament Reconstruction-Thinking From the Endpoint
Abstract
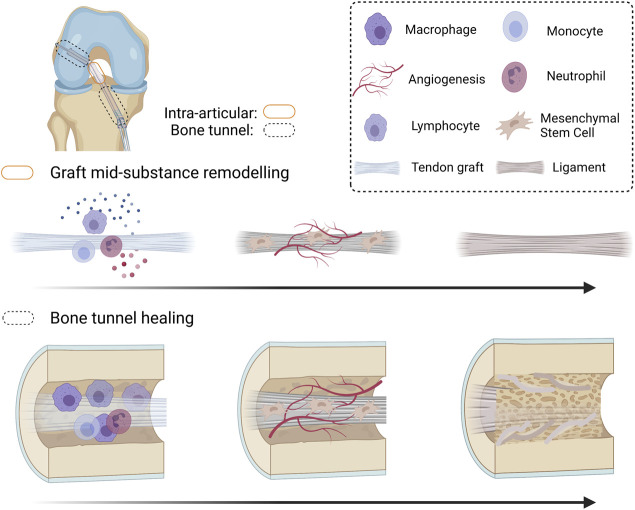
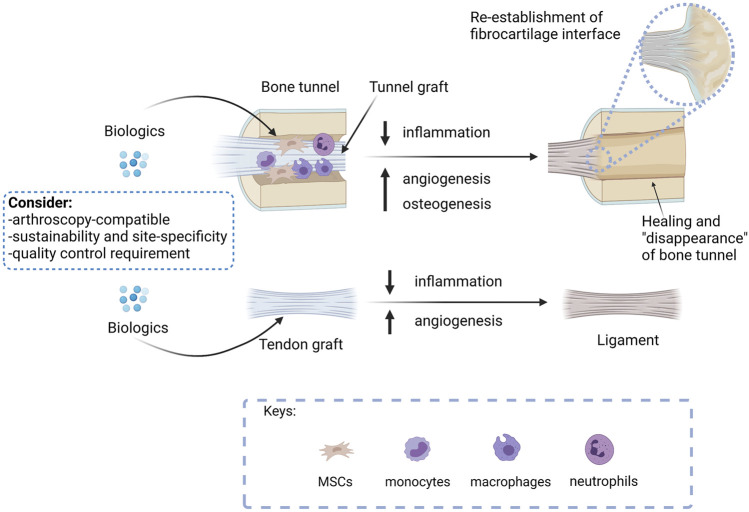
Anterior cruciate ligament (ACL) tear is common in sports and accidents, and accounts for over 50% of all knee injuries. ACL reconstruction (ACLR) is commonly indicated to restore the knee stability, prevent anterior-posterior translation, and reduce the risk of developing post-traumatic osteoarthritis. However, the outcome of biological graft healing is not satisfactory with graft failure after ACLR. Tendon graft-to-bone tunnel healing and graft mid-substance remodeling are two key challenges of biological graft healing after ACLR. Mounting evidence supports excessive inflammation due to ACL injury and ACLR, and tendon graft-to-bone tunnel motion negatively influences these two key processes. To tackle the problem of biological graft healing, we believe that an inductive approach should be adopted, starting from the endpoint that we expected after ACLR, even though the results may not be achievable at present, followed by developing clinically practical strategies to achieve this ultimate goal. We believe that mineralization of tunnel graft and ligamentization of graft mid-substance to restore the ultrastructure and anatomy of the original ACL are the ultimate targets of ACLR. Hence, strategies that are osteoinductive, angiogenic, or anti-inflammatory should drive graft healing toward the targets. This paper reviews pre-clinical and clinical literature supporting this claim and the role of inflammation in negatively influencing graft healing. The practical considerations when developing a biological therapy to promote ACLR for future clinical translation are also discussed.
Keywords: ACL; ACL reconstruction; angiogenesis; anterior cruciate ligament; biological therapy; graft healing; inflammation; osteogenesis.
Copyright © 2021 Yao, Yung and Lui.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Brophy R. H., Kovacevic D., Imhauser C. W., Stasiak M., Bedi A., Fox A. J., et al. (2011). Effect of Short-Duration Low-Magnitude Cyclic Loading versus Immobilization on Tendon-Bone Healing after ACL Reconstruction in a Rat Model. The J. Bone Jt. Surgery-American Volume 93 (4), 381–393. 10.2106/jbjs.I.00933 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources