

Effectiveness of Combined Strategies for the Prevention of Hypothermia Measured by Noninvasive Zero-Heat Flux Thermometer During Cesarean Section
- PMID: 35004715
- PMCID: PMC8732358
- DOI: 10.3389/fmed.2021.734768
Effectiveness of Combined Strategies for the Prevention of Hypothermia Measured by Noninvasive Zero-Heat Flux Thermometer During Cesarean Section
Abstract
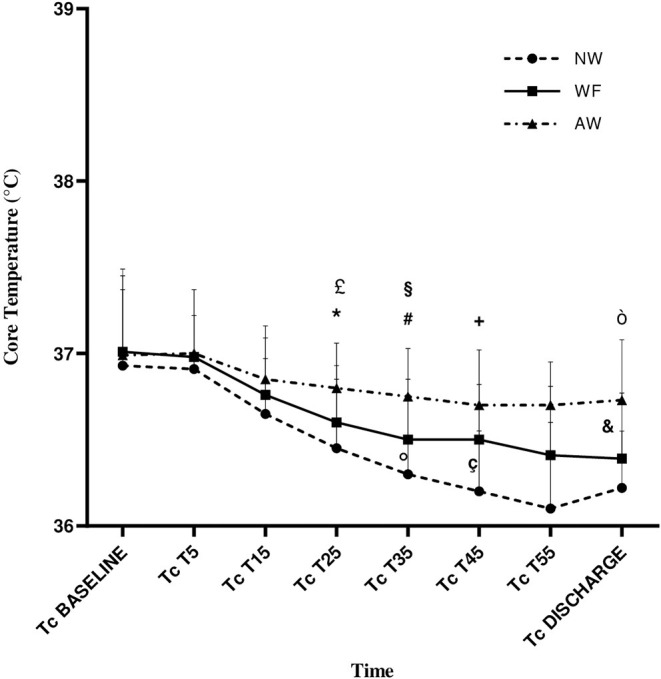
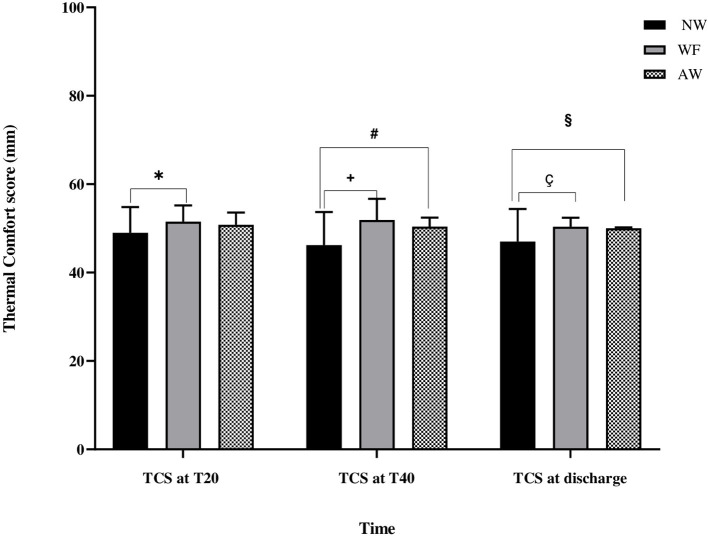
Background: Perioperative hypothermia (body temperature <36°C) is a common complication of anesthesia increasing the risk for maternal cardiovascular events and coagulative disorders, and can also influence neonatal health. The aim of our work was to evaluate the impact of combined warming strategies on maternal core temperature, measured with the SpotOn. We hypothesized that combined modalities of active warming prevent hypothermia in pregnant women undergoing cesarean delivery with spinal anesthesia. Methods: Seventy-eight pregnant women were randomly allocated into three study groups receiving warmed IV fluids and forced-air warming (AW), warmed IV fluids (WF), or no warming (NW). Noninvasive core temperature device (SpotOn) measured maternal core temperature intraoperatively and for 30 min after surgery. Maternal mean arterial pressure, incidence of shivering, thermal comfort and newborn's APGAR, axillary temperature, weight, and blood gas analysis were also recorded. Results: Incidence of hypothermia was of 0% in AW, 4% in WF, and 47% in NW. Core temperature in AW was constantly higher than WF and NW groups. Incidence of shivering in perioperative time was significantly lower in AW and WF groups compared with the NW group (p < 0.04). Thermal comfort was higher in both AW and WF groups compared with NW group (p = 0.02 and p = 0.008, respectively). There were no significant differences among groups for the other evaluated parameters. Conclusion: Combined modalities of active warming are effective in preventing perioperative hypothermia. The routine uses of combined AW are suggested in the setting of cesarean delivery.
Keywords: SpotOn; cesarean delivery (CD); core temperature; perioperative hypothermia; spinal anesthesia.
Copyright © 2021 Cotoia, Mariotti, Ferialdi, Del Vecchio, Beck, Zaami and Cinnella.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Active Warming Utilizing Combined IV Fluid and Forced-Air Warming Decreases Hypothermia and Improves Maternal Comfort During Cesarean Delivery: A Randomized Control Trial.Anesth Analg. 2016 May;122(5):1490-7. doi: 10.1213/ANE.0000000000001181. Anesth Analg. 2016. PMID: 26895002 Clinical Trial.
-
Effects of combined warmed preoperative forced-air and warmed perioperative intravenous fluids on maternal temperature during cesarean section: a prospective, randomized, controlled clinical trial.BMC Anesthesiol. 2020 Feb 26;20(1):48. doi: 10.1186/s12871-020-00970-7. BMC Anesthesiol. 2020. PMID: 32101145 Free PMC article. Clinical Trial.
-
Efficacy of forced-air warming and warmed intravenous fluid for prevention of hypothermia and shivering during caesarean delivery under spinal anaesthesia: A randomised controlled trial.Eur J Anaesthesiol. 2019 Jun;36(6):442-448. doi: 10.1097/EJA.0000000000000990. Eur J Anaesthesiol. 2019. PMID: 30985539 Clinical Trial.
-
Effect of active and passive warming on preventing hypothermia and shivering during cesarean delivery: a systematic review and meta-analysis of randomized controlled trials.BMC Pregnancy Childbirth. 2022 Sep 21;22(1):720. doi: 10.1186/s12884-022-05054-7. BMC Pregnancy Childbirth. 2022. PMID: 36131231 Free PMC article.
-
The Effect of patient warming during Caesarean delivery on maternal and neonatal outcomes: a meta-analysis.Br J Anaesth. 2015 Oct;115(4):500-10. doi: 10.1093/bja/aev325. Br J Anaesth. 2015. PMID: 26385660 Free PMC article. Review.
Cited by
-
Consensus on the Southeast Asian management of hypotension using vasopressors and adjunct modalities during cesarean section under spinal anesthesia.J Anesth Analg Crit Care. 2022 Dec 28;2(1):56. doi: 10.1186/s44158-022-00084-1. J Anesth Analg Crit Care. 2022. PMID: 37386598 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources