

Molecular Mechanisms of Proteinuria in Minimal Change Disease
- PMID: 35004732
- PMCID: PMC8733331
- DOI: 10.3389/fmed.2021.761600
Molecular Mechanisms of Proteinuria in Minimal Change Disease
Abstract
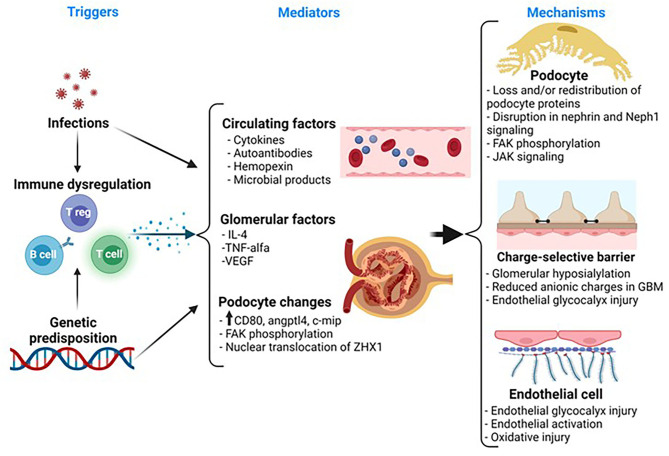
Minimal change disease (MCD) is the most common type of idiopathic nephrotic syndrome in childhood and represents about 15% cases in adults. It is characterized by massive proteinuria, edema, hypoalbuminemia, and podocyte foot process effacement on electron microscopy. Clinical and experimental studies have shown an association between MCD and immune dysregulation. Given the lack of inflammatory changes or immunocomplex deposits in the kidney tissue, MCD has been traditionally thought to be mediated by an unknown circulating factor(s), probably released by T cells that directly target podocytes leading to podocyte ultrastructural changes and proteinuria. Not surprisingly, research efforts have focused on the role of T cells and podocytes in the disease process. Nevertheless, the pathogenesis of the disease remains a mystery. More recently, B cells have been postulated as an important player in the disease either by activating T cells or by releasing circulating autoantibodies against podocyte targets. There are also few reports of endothelial injury in MCD, but whether glomerular endothelial cells play a role in the disease remains unexplored. Genome-wide association studies are providing insights into the genetic susceptibility to develop the disease and found a link between MCD and certain human haplotype antigen variants. Altogether, these findings emphasize the complex interplay between the immune system, glomerular cells, and the genome, raising the possibility of distinct underlying triggers and/or mechanisms of proteinuria among patients with MCD. The heterogeneity of the disease and the lack of good animal models of MCD remain major obstacles in the understanding of MCD. In this study, we will review the most relevant candidate mediators and mechanisms of proteinuria involved in MCD and the current models of MCD-like injury.
Keywords: circulating factor; immune cell; minimal change disease; nephrotic syndrome; podocyte; proteinuria.
Copyright © 2021 Purohit, Piani, Ordoñez, de Lucas-Collantes, Bauer and Cara-Fuentes.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- The primary nephrotic syndrome in children . Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. J Pediatr. (1981) 98:561–4. - PubMed
-
- Cameron JS. Nephrotic syndrome in the elderly. Semin Nephrol. (1996) 16:319–29. - PubMed
Publication types
LinkOut - more resources
Full Text Sources