

Survival Outcomes and Prognostic Predictors in Patients With Malignant Struma Ovarii
- PMID: 35004743
- PMCID: PMC8733601
- DOI: 10.3389/fmed.2021.774691
Survival Outcomes and Prognostic Predictors in Patients With Malignant Struma Ovarii
Abstract
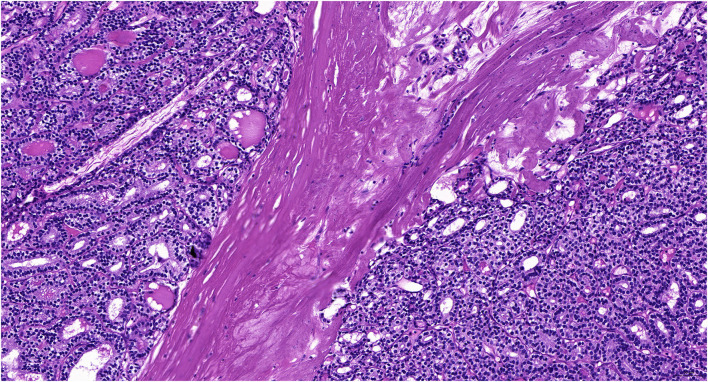
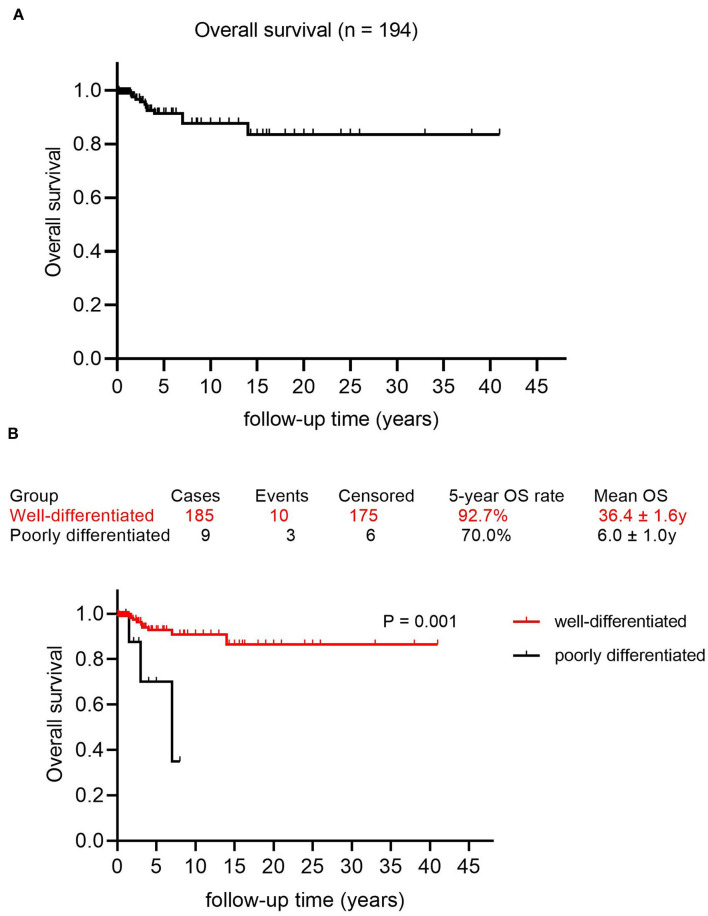
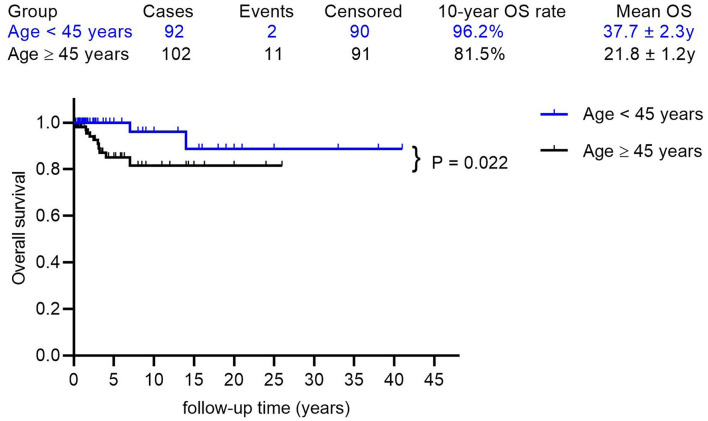
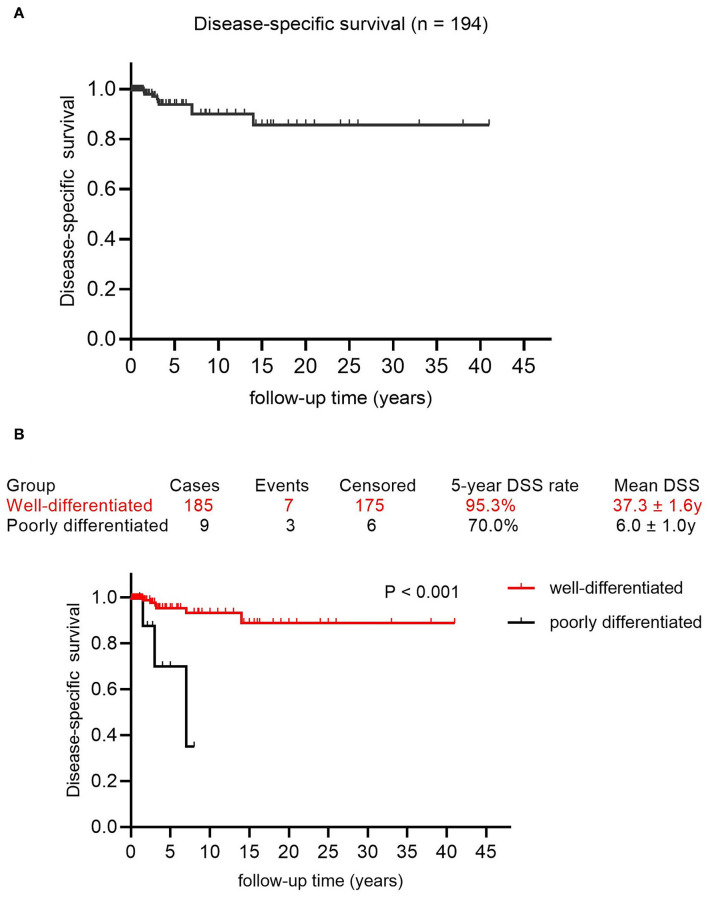
Background: Malignant struma ovarii (MSO) is an extremely rare ovarian malignant tumor and there is limited data on the survival outcomes and prognostic predictors of MSO. The objectives of this study were to investigate the disease-free survival (DFS), overall survival (OS), and disease-specific survival (DSS) rates of patients with MSO, and also evaluate the prognostic factors in this population. Methods: A retrospective study was conducted and 194 cases of MSO were selected. DFS was assessed by the logistic regression, OS by the Kaplan-Meier method, and DSS was evaluated by the Cox regression. Results: The median age of these patients was 46.0 years; 142 cases (73.2%) were confined to the ovary and 52 cases (26.8%) had extraovarian metastasis at the initial diagnosis of MSO. During the follow-up, 75.3% of these patients showed no evidence of disease and 18.0% were alive with disease. Only 13 deaths occurred, with 10 attributed to MSO. The 5, 10, and 15-year OS rates were 91.4, 87.7, and 83.5%, respectively. The 5, 10, and 15-year DSS rates were 93.8, 90.0, and 85.7%, respectively. Logistic regression revealed that International Federation of Gynecology and Obstetrics (FIGO) stage IV was the only risk factor for DFS [p < 0.001; odds ratio (OR) 7.328; 95% CI 3.103-16.885, FIGO stage IV vs. stage I; p = 0.021; OR 4.750, 95% CI 1.264-17.856, FIGO stage IV vs. stage II-III]. The multivariate Cox regression analysis showed that poor differentiation was the only risk factor for both OS (p = 0.005, OR 6.406; 95% CI 1.730-23.717) and DSS (p = 0.001, OR 9.664; 95% CI 2.409-38.760), while age ≥45 years was the prognostic predictor for OS (p = 0.038, OR 4.959; 95% CI 1.093-22.508). Conclusion: Survival outcomes were excellent in patients with MSO, irrespective of the treatment strategy, FIGO stage IV, age ≥45 years, and poor differentiation of tumors were the independent risk factors.
Keywords: malignant struma ovarii; prognostic factors; survival outcomes; thyroid carcinoma; treatment.
Copyright © 2021 Li, Kong, Wang, Zhang, Yin and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Fujiwara S, Tsuyoshi H, Nishimura T, Takahashi N, Yoshida Y. Precise preoperative diagnosis of struma ovarii with pseudo-Meigs' syndrome mimicking ovarian cancer with the combination of 131I scintigraphy and 18F–FDG PET: case report and review of the literature. J Ovarian Res. (2018) 11:11. 10.1186/s13048-018-0383-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources