

Comparison of Resting Full-Cycle Ratio and Fractional Flow Reserve in a German Real-World Cohort
- PMID: 35004875
- PMCID: PMC8740550
- DOI: 10.3389/fcvm.2021.744181
Comparison of Resting Full-Cycle Ratio and Fractional Flow Reserve in a German Real-World Cohort
Abstract
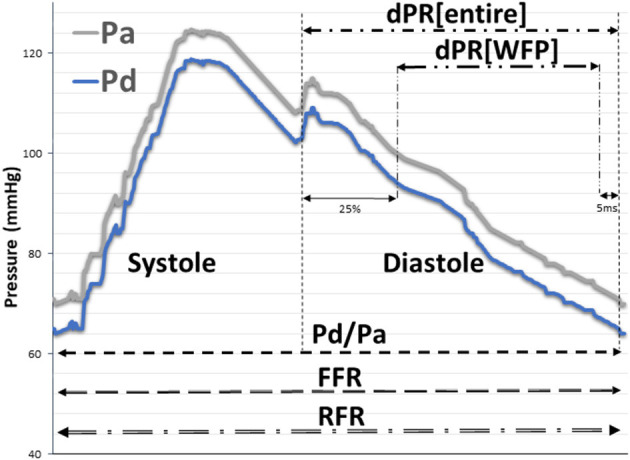
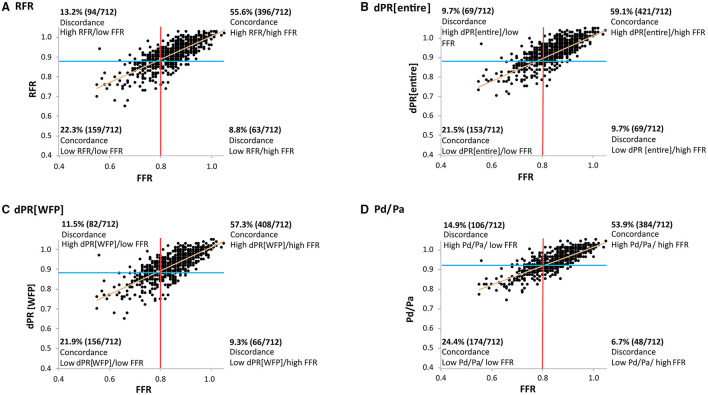
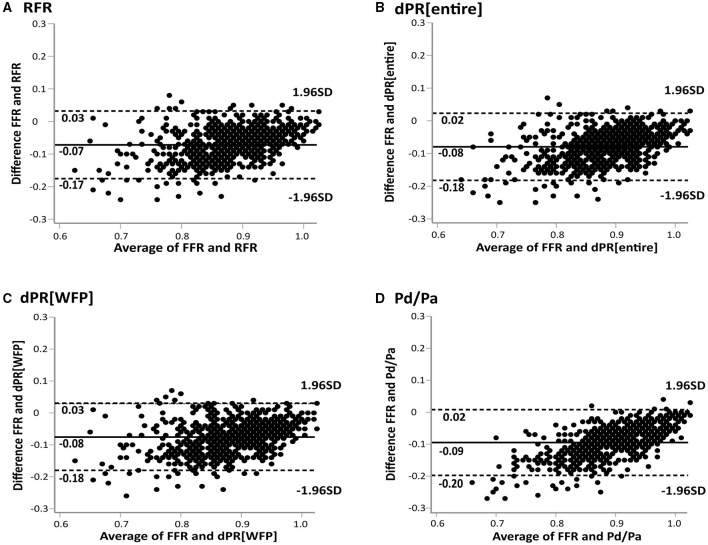
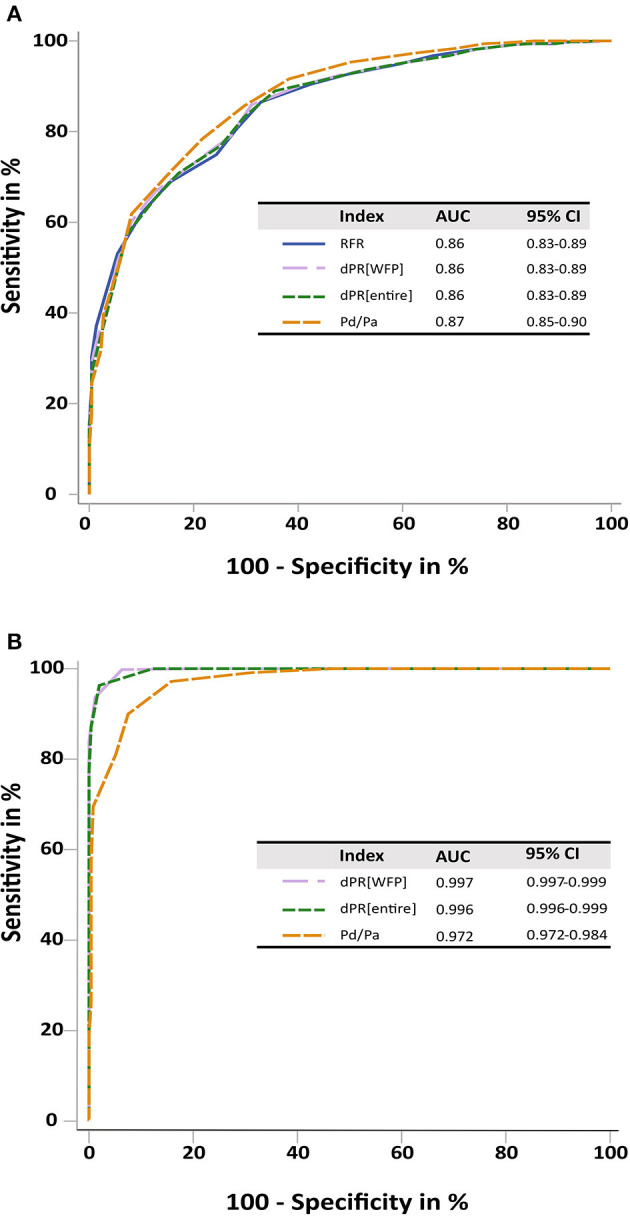
Objective: The aim of this study was to evaluate non-hyperemic resting pressure ratios (NHPRs), especially the novel "resting full-cycle ratio" (RFR; lowest pressure distal to the stenosis/aortic pressure during the entire cardiac cycle), compared to the gold standard fractional flow reserve (FFR) in a "real-world" setting. Methods: The study included patients undergoing coronary pressure wire studies at one German University Hospital. No patients were excluded based on any baseline or procedural characteristics, except for insufficient quality of traces. The diagnostic performance of four NHPRs vs. FFR ≤ 0.80 was tested. Morphological characteristics of stenoses were analyzed by quantitative coronary angiography. Results: 617 patients with 712 coronary lesions were included. RFR showed a significant correlation with FFR (r = 0.766, p < 0.01). Diagnostic accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of RFR were 78% (95% confidence interval = 75; 81), 72% (65; 78), 81% (77; 84), 63% (57; 69), and 86% (83; 89). Relevant predictors for discordance of RFR ≤ 0.89/FFR > 0.8 were LAD lesions, peripheral artery disease, age, female sex and non-focal stenoses. Predictors for discordance of RFR > 0.89/FFR ≤ 0.8 included non-LCX lesions, percent diameter stenosis and previous percutaneous coronary intervention in the target vessel. RFR and all other NHPRs were highly correlated with each other. Conclusion: All NHPRs have a similar correlation with the gold standard FFR and may facilitate the acceptance and implementation of physiological assessments of lesion severity. However, we found ~20% discordant results between NHPRs and FFR in our "all-comers" German cohort.
Keywords: coronary artery disease (CAD); coronary physiology; fractional flow reserve (FFR); invasive coronary angiography (ICA); resting full-cycle ratio (RFR).
Copyright © 2021 Wienemann, Meyer, Mauri, Baar, Adam, Baldus and Halbach.
Conflict of interest statement
SB and MH received institutional grant support and speakers' honoraria from Abbott Vascular. HW received institutional grant support from Abbott Vascular. Abbott Vascular had no influence on the design of the study, data analysis or interpretation of findings. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Zimmermann FM, Ferrara A, Johnson NP, van Nunen LX, Escaned J, Albertsson P, et al. Deferral vs. performance of percutaneous coronary intervention of functionally non-significant coronary stenosis: 15-year follow-up of the DEFER trial. Eur Heart J. (2015) 36:3182–8. 10.1093/eurheartj/ehv452 - DOI - PubMed
-
- van Nunen LX, Zimmermann FM, Tonino PA, Barbato E, Baumbach A, Engstrøm T, et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet. (2015) 386:1853–60. 10.1016/S0140-6736(15)00057-4 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous