

A Phenotyping of Diastolic Function by Machine Learning Improves Prediction of Clinical Outcomes in Heart Failure
- PMID: 35004877
- PMCID: PMC8733156
- DOI: 10.3389/fcvm.2021.755109
A Phenotyping of Diastolic Function by Machine Learning Improves Prediction of Clinical Outcomes in Heart Failure
Abstract
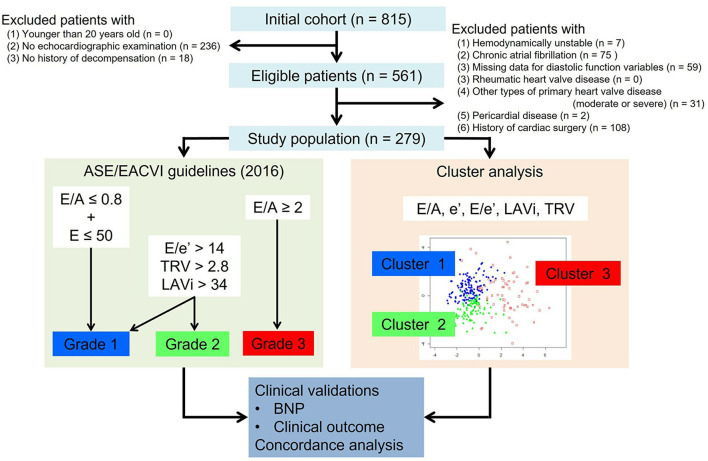
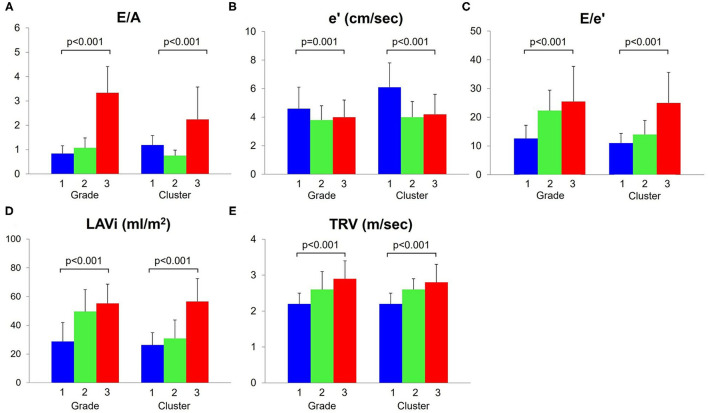
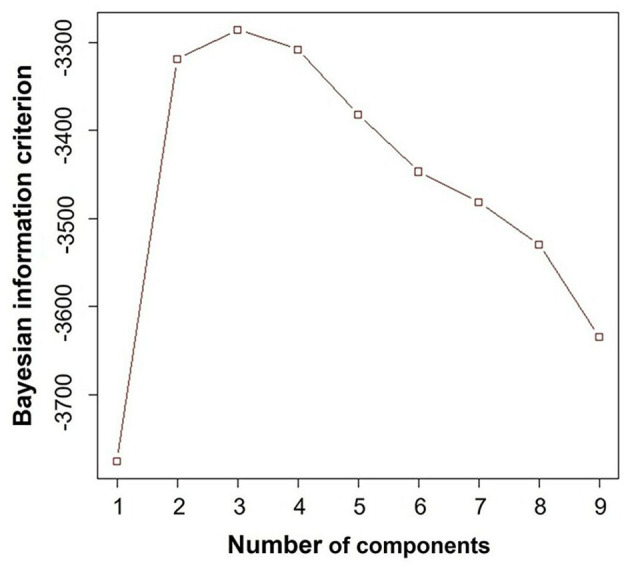
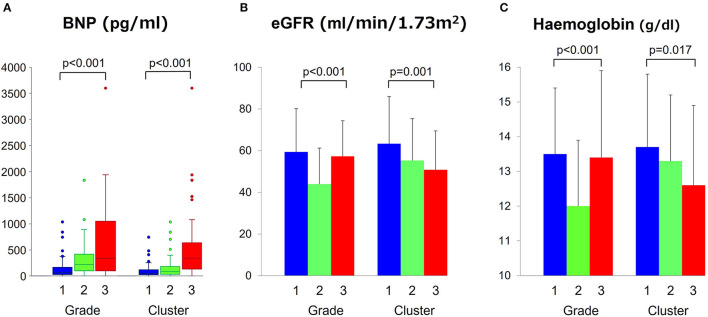
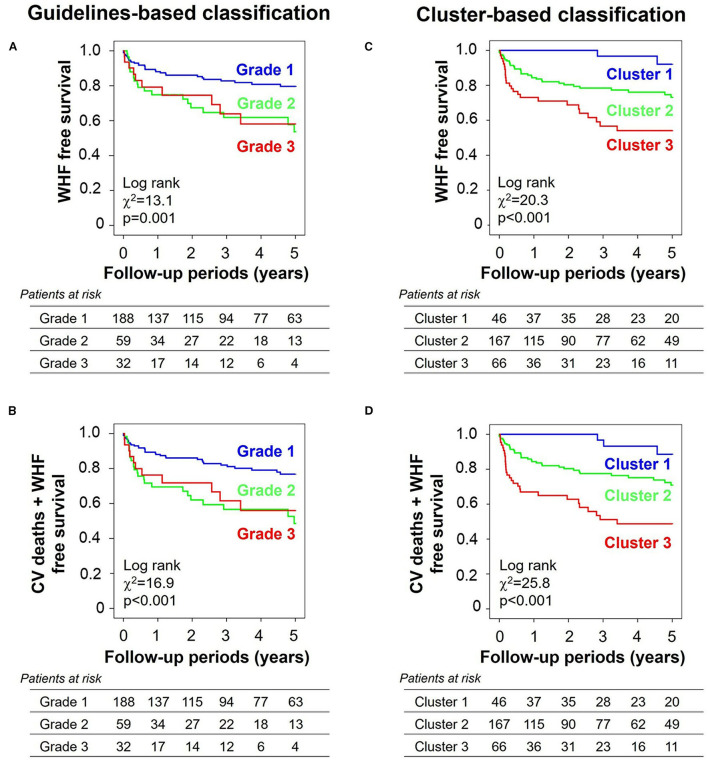
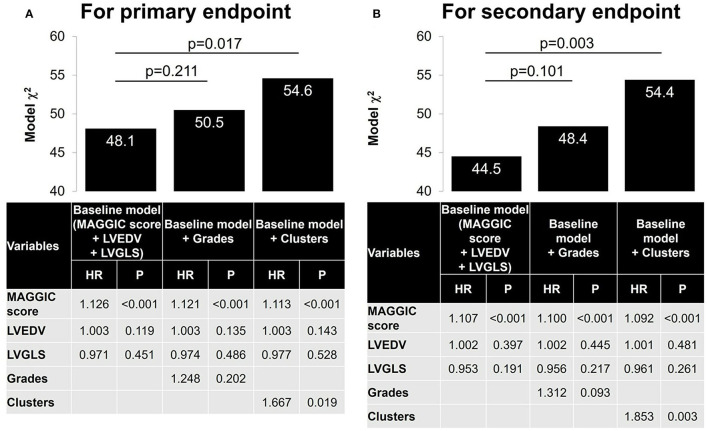
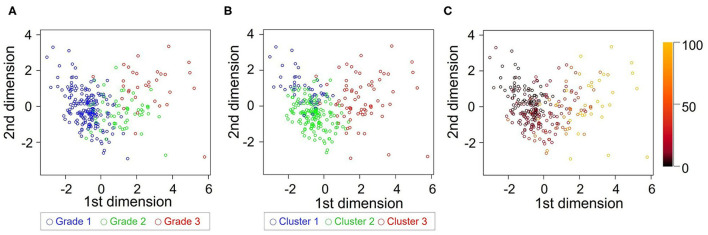
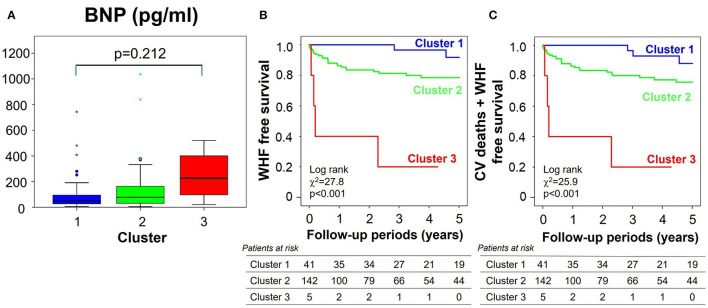
Background: Discriminating between different patterns of diastolic dysfunction in heart failure (HF) is still challenging. We tested the hypothesis that an unsupervised machine learning algorithm would detect heterogeneity in diastolic function and improve risk stratification compared with recommended consensus criteria. Methods: This study included 279 consecutive patients aged 24-97 years old with clinically stable HF referred for echocardiographic assessment, in whom diastolic variables were measured according to the current guidelines. Cluster analysis was undertaken to identify homogeneous groups of patients with similar profiles of the variables. Sequential Cox models were used to compare cluster-based classification with guidelines-based classification for predicting clinical outcomes. The primary endpoint was hospitalization for worsening HF. Results: The analysis identified three clusters with distinct properties of diastolic function that shared similarities with guidelines-based classification. The clusters were associated with brain natriuretic peptide level (p < 0.001), hemoglobin concentration (p = 0.017) and estimated glomerular filtration rate (p = 0.001). During a mean follow-up period of 2.6 ± 2.0 years, 62 patients (22%) experienced the primary endpoint. Cluster-based classification predicted events with a hazard ratio 1.68 (p = 0.019) that was independent from and incremental to the Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) risk score for HF, and from left ventricular end-diastolic volume and global longitudinal strain, whereas guidelines-based classification did not retain its independent prognostic value (hazard ratio = 1.25, p = 0.202). Conclusion: Machine learning can identify patterns of diastolic function that better stratify the risk for decompensation than the current consensus recommendations in HF. Integrating this data-driven phenotyping may help in refining prognostication and optimizing treatment.
Keywords: diastolic function; echocardiogram classification; heart failure; machine learning; prognostication factor.
Copyright © 2021 Kameshima, Uejima, Fraser, Takahashi, Cho, Suzuki, Kato, Yajima and Yamashita.
Conflict of interest statement
TU received a research funding from Hitachi. SS received a lecture fee from Daiichi-Sankyo and a research funding from Daiichi-Sankyo and Mitsubishi-Tanabe. TY has received a research funding from Daiichi-Sankyo, Bayer Healthcare, and Bristol Meyers Squibb and a remuneration from Daiichi-Sankyo, Pfizer, Bayer Healthcare, Bristol-Myers Squibb, Toa Eiyo, and Ono Pharmaceutical. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Left Atrial Strain in the Assessment of Diastolic Function in Heart Failure: A Machine Learning Approach.Circ Cardiovasc Imaging. 2023 Feb;16(2):e014605. doi: 10.1161/CIRCIMAGING.122.014605. Epub 2023 Feb 8. Circ Cardiovasc Imaging. 2023. PMID: 36752112
-
Phenotypic Clustering of Left Ventricular Diastolic Function Parameters: Patterns and Prognostic Relevance.JACC Cardiovasc Imaging. 2019 Jul;12(7 Pt 1):1149-1161. doi: 10.1016/j.jcmg.2018.02.005. Epub 2018 Apr 18. JACC Cardiovasc Imaging. 2019. PMID: 29680357
-
Association of Abnormal Left Ventricular Functional Reserve With Outcome in Heart Failure With Preserved Ejection Fraction.JACC Cardiovasc Imaging. 2018 Dec;11(12):1737-1746. doi: 10.1016/j.jcmg.2017.07.028. Epub 2017 Nov 15. JACC Cardiovasc Imaging. 2018. PMID: 29153571
-
Prognostic value of N-terminal pro-type-B natriuretic peptide and Doppler left ventricular diastolic variables in patients with chronic systolic heart failure stabilized by therapy.Am J Cardiol. 2008 Aug 15;102(4):463-8. doi: 10.1016/j.amjcard.2008.03.083. Epub 2008 May 24. Am J Cardiol. 2008. PMID: 18678307
-
Meta-Analysis Global Group in Chronic (MAGGIC) Heart Failure Risk Score: Validation of a Simple Tool for the Prediction of Morbidity and Mortality in Heart Failure With Preserved Ejection Fraction.J Am Heart Assoc. 2018 Oct 16;7(20):e009594. doi: 10.1161/JAHA.118.009594. J Am Heart Assoc. 2018. PMID: 30371285 Free PMC article.
References
-
- Somaratne JB, Whalley GA, Gamble GD, Doughty RN. Restrictive filling pattern is a powerful predictor of heart failure events postacute myocardial infarction and in established heart failure: a literature-based meta-analysis. J Card Fail. (2007) 13:346–52. 10.1016/j.cardfail.2007.01.010 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous