

Center-To-Periphery Arterial Stiffness Gradient Is Attenuated and/or Reversed in Pregnancy-Associated Hypertension
- PMID: 35004884
- PMCID: PMC8739768
- DOI: 10.3389/fcvm.2021.766723
Center-To-Periphery Arterial Stiffness Gradient Is Attenuated and/or Reversed in Pregnancy-Associated Hypertension
Abstract
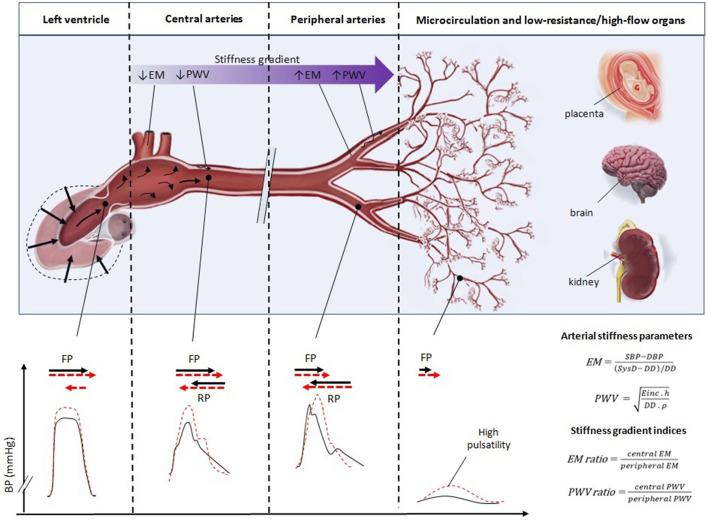
Background: Non-pregnant (NP) women have a progressive increase in arterial stiffness from central-to-peripheral arteries ["stiffness gradient" (SG)], which is of physiologic importance since excessive pulsatility is filtered by the creation of wave reflections. If the aorta gets stiff with minimal or no change in the periphery, the SG is dissipated transmitting pressure disturbances to the microcirculation. It remains unknown the status of the SG in both women with healthy pregnancies (HP) and complicated by pregnancy-associated hypertension (PAH). Objective: To determine whether HP and PAH are associated with changes in SG. Secondarily, we aim at identifying potential differences between the subgroups of PAH (pre-eclampsia and gestational hypertension). Methods: HP (n = 10), PAH (n = 16), and healthy NP women (n = 401, to be matched for age, and cardiovascular risk with the pregnant women) were included. Carotid-to-femoral (cfPWV) and carotid-to-radial pulse wave velocity (crPWV), common carotid artery (CCA) and brachial artery (BA) diameters and elastic modulus (EM), and regional (cfPWV/crPWV or "PWV ratio") and local (CCA EM/BA EM or "EM ratio") SG were quantified. Results: HP showed no changes in PWV ratio compared with NP, in the presence of significantly lower cfPWV and crPWV. HP exhibited higher arterial diameters and lower CCA EM/BA EM compared to NP, without differences with PAH. PAH was associated with a significant increase in the PWV ratio that exceeded the levels of both NP and HP, explained by a lower (although significant) reduction of cfPWV with respect to that observed in HP with respect to NP, and a higher reduction in crPWV with respect to that observed between HP and NP. The blunted reduction in cfPWV observed in PAH coincided with an increase in the CCA EM. Conclusions: Compared with NP, HP was associated with unchanged PWV ratio but with a reduction in CCA EM/BA EM, in the setting of a generalized drop in arterial stiffness. Compared with NP and HP, PAH was associated with an "exaggerated rise" in the PWV ratio without changes in CCA EM/BA EM, in the setting of a blunt reduction in cfPWV but exaggerated crPWV drop. The SG attenuation/reversal in PAH was mainly driven by pre-eclampsia.
Keywords: arterial stiffness; carotids; gestational hypertension; pre-eclampsia; pregnancy.
Copyright © 2021 Pereira, Torrado, Sosa, Diaz, Bia and Zócalo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Physiological Age- and Sex-Related Profiles for Local (Aortic) and Regional (Carotid-Femoral, Carotid-Radial) Pulse Wave Velocity and Center-to-Periphery Stiffness Gradient, with and without Blood Pressure Adjustments: Reference Intervals and Agreement between Methods in Healthy Subjects (3-84 Years).J Cardiovasc Dev Dis. 2021 Jan 12;8(1):3. doi: 10.3390/jcdd8010003. J Cardiovasc Dev Dis. 2021. PMID: 33445548 Free PMC article.
-
A longitudinal analysis of arterial stiffness and wave reflection in preeclampsia: Identification of changepoints.Metabolism. 2021 Jul;120:154794. doi: 10.1016/j.metabol.2021.154794. Epub 2021 May 8. Metabolism. 2021. PMID: 33971204
-
Utility of Estimated Pulse Wave Velocity for Tracking the Arterial Response to Prolonged Sitting.J Cardiovasc Dev Dis. 2022 Nov 23;9(12):411. doi: 10.3390/jcdd9120411. J Cardiovasc Dev Dis. 2022. PMID: 36547408 Free PMC article.
-
[The changes and impact factors of carotid-femoral and carotid-radial pulse wave velocity in patients with essential hypertension].Zhonghua Xin Xue Guan Bing Za Zhi. 2005 Dec;33(12):1088-91. Zhonghua Xin Xue Guan Bing Za Zhi. 2005. PMID: 16563276 Chinese.
-
Arterial Stiffness Gradient.Pulse (Basel). 2016 Apr;3(3-4):159-66. doi: 10.1159/000438852. Epub 2015 Sep 2. Pulse (Basel). 2016. PMID: 27195235 Free PMC article. Review.
Cited by
-
Increase of augmentation index (AIx@75): a promising tool for screening hypertensive pregnancy disorders.BMC Pregnancy Childbirth. 2025 Apr 16;25(1):457. doi: 10.1186/s12884-025-07493-4. BMC Pregnancy Childbirth. 2025. PMID: 40240985 Free PMC article.
-
The Impact of Medical Physical Training and a Structured Personalized Exercise Training Program on Hemodynamic Parameters and Arterial Stiffness in Pregnant Women.Biomedicines. 2024 Apr 30;12(5):986. doi: 10.3390/biomedicines12050986. Biomedicines. 2024. PMID: 38790947 Free PMC article.
-
Wave separation analysis-derived indexes obtained from radial and carotid tonometry in healthy pregnancy and pregnancy-associated hypertension: Comparison with pulse wave analysis-derived indexes.Front Cardiovasc Med. 2022 Nov 1;9:997452. doi: 10.3389/fcvm.2022.997452. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36386340 Free PMC article.
-
Relationship between the structure, function and endothelial damage, and vascular ageing and the biopsychological situation in adults diagnosed with persistent COVID (BioICOPER study). A research protocol of a cross-sectional study.Front Physiol. 2023 Sep 12;14:1236430. doi: 10.3389/fphys.2023.1236430. eCollection 2023. Front Physiol. 2023. PMID: 37772064 Free PMC article.
-
Development of non-invasive biomarkers for pre-eclampsia through data-driven cardiovascular network models.Sci Rep. 2024 Oct 4;14(1):23144. doi: 10.1038/s41598-024-72832-y. Sci Rep. 2024. PMID: 39367038 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous