

Aortic Pressure Levels and Waveform Indexes in People Living With Human Immunodeficiency Virus: Impact of Calibration Method on the Differences With Respect to Non-HIV Subjects and Optimal Values
- PMID: 35004887
- PMCID: PMC8733318
- DOI: 10.3389/fcvm.2021.772912
Aortic Pressure Levels and Waveform Indexes in People Living With Human Immunodeficiency Virus: Impact of Calibration Method on the Differences With Respect to Non-HIV Subjects and Optimal Values
Abstract
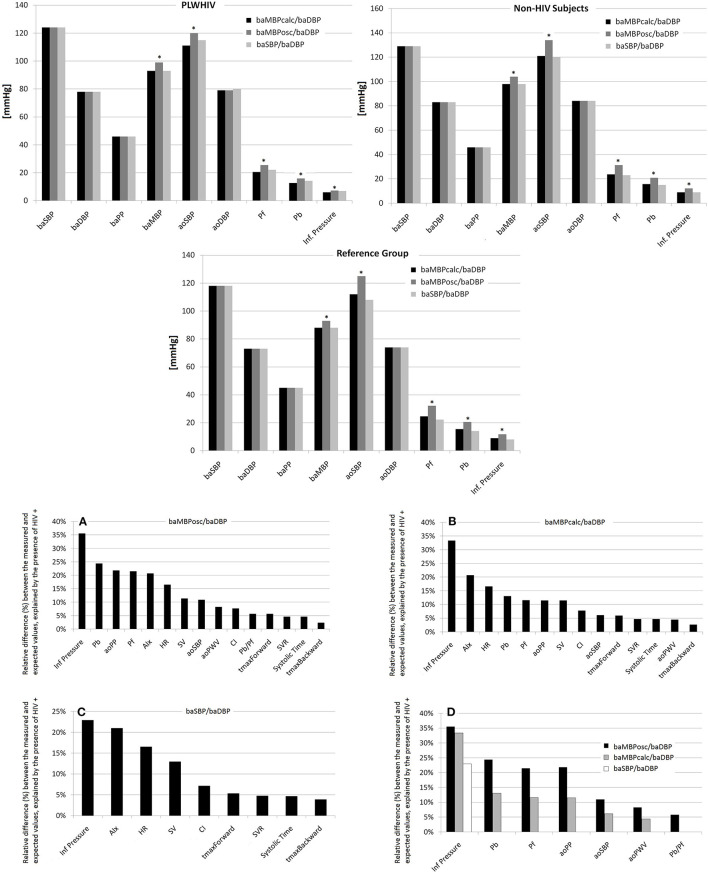
Background: There are scarce and controversial data on whether human immunodeficiency virus (HIV) infection is associated with changes in aortic pressure (aoBP) and waveform-derived indexes. Moreover, it remains unknown whether potential differences in aoBP and waveform indexes between people living with HIV (PLWHIV) and subjects without HIV (HIV-) would be affected by the calibration method of the pressure waveform. Aims: To determine: (i) whether PLWHIV present differences in aoBP and waveform-derived indexes compared to HIV- subjects; (ii) the relative impact of both HIV infection and cardiovascular risk factors (CRFs) on aoBP and waveform-derived indexes; (iii) whether the results of the first and second aims are affected by the calibration method. Methods: Three groups were included: (i) PLWHIV (n = 86), (ii) HIV- subjects (general population; n = 1,000) and (iii) a Reference Group (healthy, non-exposed to CRFs; n = 398). Haemodynamic parameters, brachial pressure (baBP; systolic: baSBP; diastolic: baDBP; mean oscillometric: baMBPosc) and aoBP and waveform-derived indexes were obtained. Brachial mean calculated (baMBPcalc=baDBP+[baSBP-baDBP]/3) pressure was quantified. Three waveform calibration schemes were used: systolic-diastolic, calculated (baMBPcalc/baDBP) and oscillometric mean (baMBPosc/baDBP). Results: Regardless of CRFs and baBP, PLWHIV presented a tendency of having lower aoBP and waveform-derived indexes which clearly reached statistical significance when using the baMBPosc/baDBP or baMBPcalc/baDBP calibration. HIV status exceeded the relative weight of other CRFs as explanatory variables, being the main explanatory variable for variations in central hemodynamics when using the baMBPosc/baDBP, followed by the baMBPcalc/baDBP calibration. Conclusions: The peripheral waveform calibration approach is an important determinant to reveal differences in central hemodynamics in PLWHIV.
Keywords: aortic pressure; calibration; human immunodeficiency virus; pulse contour analysis; pulse wave analysis; wave separation analysis.
Copyright © 2021 Diaz, Grand, Torrado, Salazar, Zócalo and Bia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources