

Innovative Approaches to Assess Intermediate Cardiovascular Risk Subjects: A Review From Clinical to Metabolomics Strategies
- PMID: 35004898
- PMCID: PMC8727773
- DOI: 10.3389/fcvm.2021.788062
Innovative Approaches to Assess Intermediate Cardiovascular Risk Subjects: A Review From Clinical to Metabolomics Strategies
Abstract
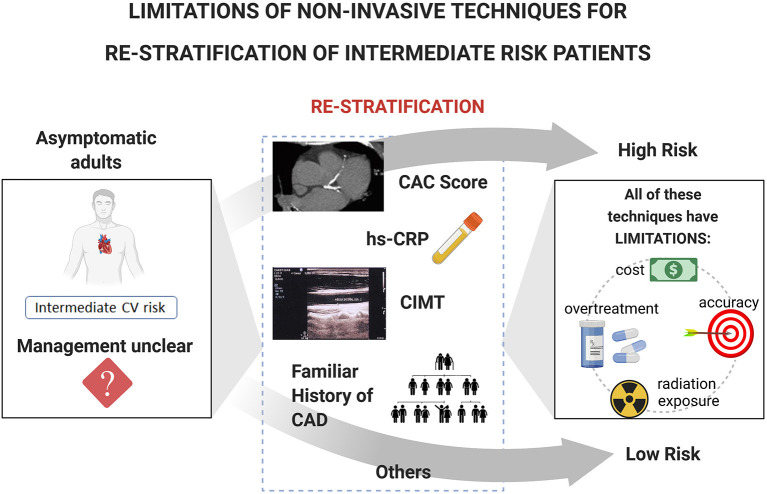
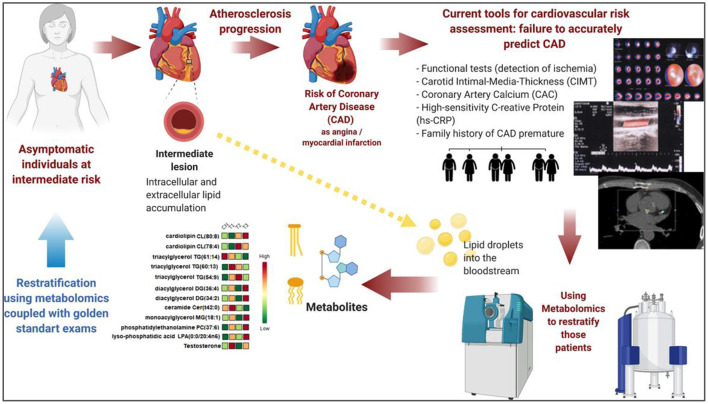
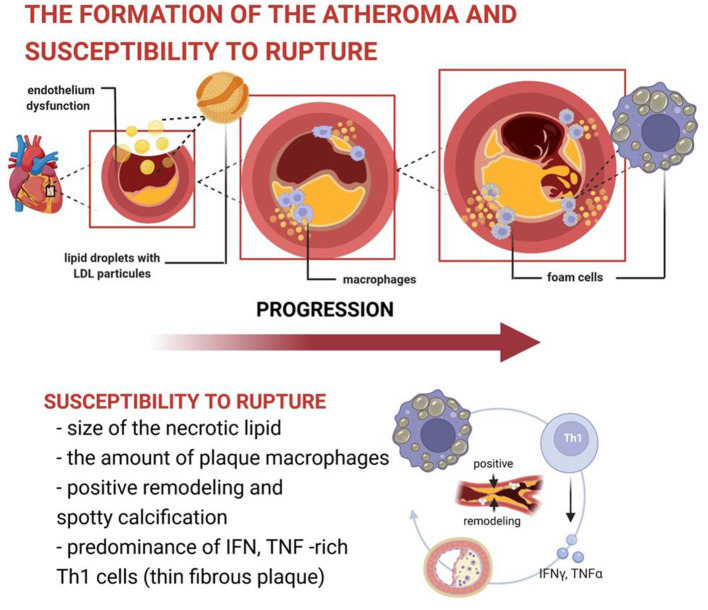
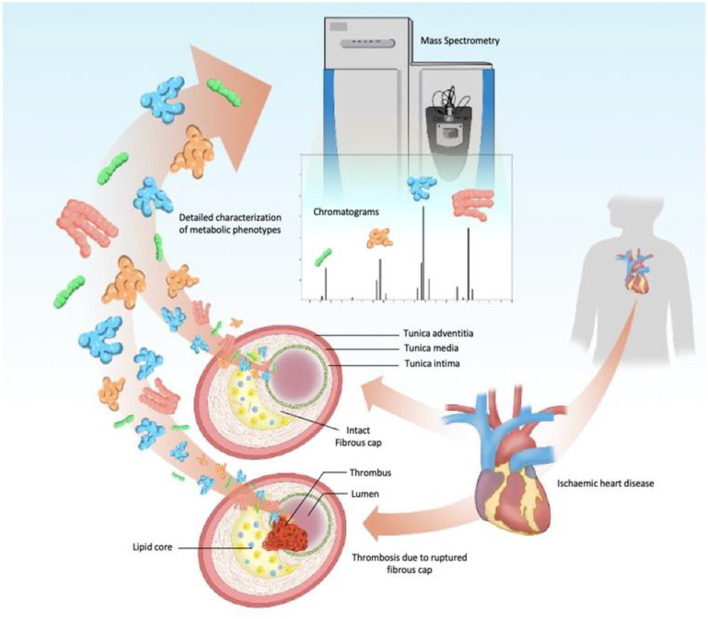
Current risk stratification strategies for coronary artery disease (CAD) have low predictive value in asymptomatic subjects classified as intermediate cardiovascular risk. This is relevant because not all coronary events occur in individuals with traditional multiple risk factors. Most importantly, the first manifestation of the disease may be either sudden cardiac death or acute coronary syndrome, after rupture and thrombosis of an unstable non-obstructive atherosclerotic plaque, which was previously silent. The inaccurate stratification using the current models may ultimately subject the individual to excessive or insufficient preventive therapies. A breakthrough in the comprehension of the molecular mechanisms governing the atherosclerosis pathology has driven many researches toward the necessity for a better risk stratification. In this Review, we discuss how metabolomics screening integrated with traditional risk assessments becomes a powerful approach to improve non-invasive CAD subclinical diagnostics. In addition, this Review highlights the findings of metabolomics studies performed by two relevant analytical platforms in current use-mass spectrometry (MS) hyphenated to separation techniques and nuclear magnetic resonance spectroscopy (NMR) -and evaluates critically the challenges for further clinical implementation of metabolomics data. We also discuss the modern understanding of the pathophysiology of atherosclerosis and the limitations of traditional analytical methods. Our aim is to show how discriminant metabolites originated from metabolomics approaches may become promising candidate molecules to aid intermediate risk patient stratification for cardiovascular events and how these tools could successfully meet the demands to translate cardiovascular metabolic biomarkers into clinical settings.
Keywords: atherosclerosis; cardiovascular prevention; coronary artery disease (CAD); metabolomics; risk stratification.
Copyright © 2021 Martins, Paiva, Paiva, de Oliveira, Machado, Alves, Picossi, Faccio, Tavares, Barbas, Giraldez, Santos, Monte and Atik.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. . 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation. (2019) 140:596–646. 10.1161/CIR.0000000000000725 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous