

Rotational Thromboelastometry in High-Risk Patients on Dual Antithrombotic Therapy After Percutaneous Coronary Intervention
- PMID: 35004899
- PMCID: PMC8727359
- DOI: 10.3389/fcvm.2021.788137
Rotational Thromboelastometry in High-Risk Patients on Dual Antithrombotic Therapy After Percutaneous Coronary Intervention
Abstract
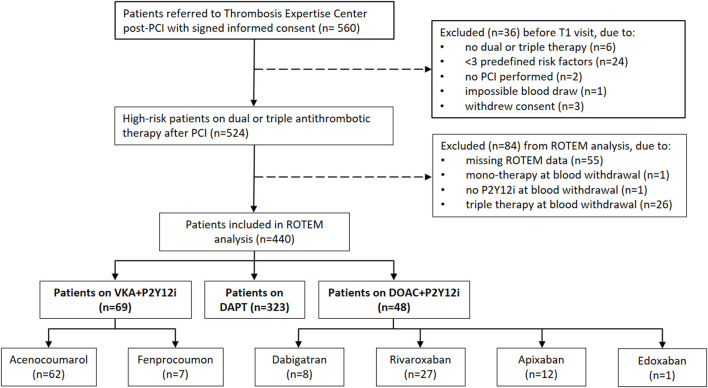
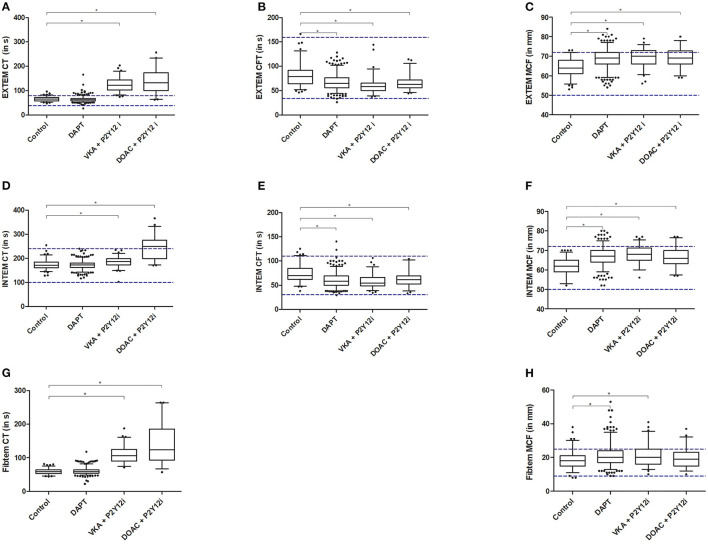
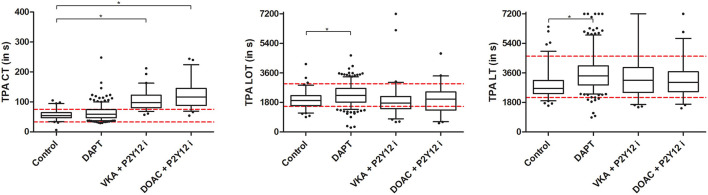
Aims: Patients using antithrombotic drugs after percutaneous coronary intervention (PCI) are at risk for bleeding and recurrent ischemia. We aimed to explore routine and tissue plasminogen activated (tPA) ROTEM results in a post-PCI population on dual antithrombotic treatment. Methods and Results: In this prospective cohort, 440 patients treated with double antithrombotic therapy after recent PCI and with ≥3 risk factors for either ischemic or bleeding complications were included and compared with a control group (n = 95) consisting of perioperative patients not using antithrombotic medication. Laboratory assessment, including (tPA) ROTEM, was performed one month post-PCI and bleeding/ischemic complications were collected over a five-month follow-up. Patients were stratified by antithrombotic regimen consisting of a P2Y12 inhibitor with either aspirin (dual antiplatelet therapy; DAPT, n = 323), a vitamin K antagonist (VKA, n = 69) or a direct oral anticoagulant (DOAC, n = 48). All post-PCI patients had elevated ROTEM clot stiffness values, but only the DAPT group additionally presented with a decreased fibrinolytic potential as measured with tPA ROTEM. Patients receiving anticoagulants had prolonged clotting times (CT) when compared to the control and DAPT group; EXTEM and FIBTEM CT could best discriminate between patients (not) using anticoagulants (AUC > 0.97). Furthermore, EXTEM CT was significantly prolonged in DAPT patients with bleeding complications during follow-up (68 [62-70] vs. 62 [57-68], p = 0.030). Conclusion: ROTEM CT has high potential for identifying anticoagulants and tPA ROTEM could detect a diminished fibrinolytic potential in patients using DAPT. Furthermore, the ability of EXTEM CT to identify patients at risk for bleeding may be promising and warrants further research.
Keywords: anticoagulants; antiplatelet drug; fibrinolysis; percutaneous coronary intervention; thromboelastometry (ROTEM®).
Copyright © 2021 Hulshof, Olie, Vries, Verhezen, van der Meijden, ten Cate and Henskens.
Conflict of interest statement
RO has received research support an honoraria from Bayer, Pfizer/BMS, Leo Pharma, Portola, and Sanofi. HC has received grants from Bayer and Pfizen, is a consultant for Alveron, and a shareholder of Coagulation Profile. YH has received ROTEM cartridges free of charge for previous research not related to the current manuscript. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Serial EXTEM, FIBTEM, and tPA Rotational Thromboelastometry Observations in the Maastricht Intensive Care COVID Cohort-Persistence of Hypercoagulability and Hypofibrinolysis Despite Anticoagulation.Front Cardiovasc Med. 2021 Apr 26;8:654174. doi: 10.3389/fcvm.2021.654174. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33981736 Free PMC article.
-
Meta-analysis of Antithrombotic Therapy in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention.Am J Cardiol. 2020 Feb 15;125(4):521-527. doi: 10.1016/j.amjcard.2019.11.022. Epub 2019 Nov 19. Am J Cardiol. 2020. PMID: 31839147
-
Risk of Stroke vs. Intracerebral Hemorrhage in Patients with Non-Valvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Comparing Dual vs. Triple Antithrombotic Therapy.J Stroke Cerebrovasc Dis. 2021 Apr;30(4):105654. doi: 10.1016/j.jstrokecerebrovasdis.2021.105654. Epub 2021 Feb 10. J Stroke Cerebrovasc Dis. 2021. PMID: 33578352
-
Non-Vitamin K Oral Anticoagulants (NOAC) Versus Vitamin K Antagonists (VKA) for Atrial Fibrillation with Elective or Urgent Percutaneous Coronary Intervention: A Meta-Analysis with a Particular Focus on Combination Type.J Clin Med. 2020 Apr 14;9(4):1120. doi: 10.3390/jcm9041120. J Clin Med. 2020. PMID: 32295160 Free PMC article.
-
Antithrombotic Therapy in Patients With Atrial Fibrillation Treated With Oral Anticoagulation Undergoing Percutaneous Coronary Intervention: A North American Perspective: 2021 Update.Circulation. 2021 Feb 9;143(6):583-596. doi: 10.1161/CIRCULATIONAHA.120.050438. Epub 2021 Feb 8. Circulation. 2021. PMID: 33555916 Review.
Cited by
-
Blood Coagulation and Beyond: Position Paper from the Fourth Maastricht Consensus Conference on Thrombosis.Thromb Haemost. 2023 Aug;123(8):808-839. doi: 10.1055/a-2052-9175. Epub 2023 Mar 13. Thromb Haemost. 2023. PMID: 36913975 Free PMC article.
-
Monitoring of Antiplatelet Therapy.Methods Mol Biol. 2023;2663:381-402. doi: 10.1007/978-1-0716-3175-1_25. Methods Mol Biol. 2023. PMID: 37204725
References
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. . 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. (2011) 124:2574–609. 10.1161/CIR.0b013e31823a5596 - DOI - PubMed
-
- Lip GY, Windecker S, Huber K, Kirchhof P, Marin F, Ten Berg JM, et al. . Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on Thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS). Eur Heart J. (2014) 35:3155–79. 10.1093/eurheartj/ehu298 - DOI - PubMed
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, et al. . 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. (2019) 140:e125–e51. 10.1161/CIR.0000000000000665 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous