

Multicenter assessment of quantitative sensory testing (QST) for the detection of neuropathic-like pain responses using the topical capsaicin model
- PMID: 35005384
- PMCID: PMC8730652
- DOI: 10.1080/24740527.2018.1525682
Multicenter assessment of quantitative sensory testing (QST) for the detection of neuropathic-like pain responses using the topical capsaicin model
Abstract
Background: The use of quantitative sensory testing (QST) in multicenter studies has been quite limited, due in part to lack of standardized procedures among centers.
Aim: The aim of this study was to assess the application of the capsaicin pain model as a surrogate experimental human model of neuropathic pain in different centers and verify the variation in reports of QST measures across centers.
Methods: A multicenter study conducted by the Quebec Pain Research Network in six laboratories allowed the evaluation of nine QST parameters in 60 healthy subjects treated with topical capsaicin to model unilateral pain and allodynia. The same measurements (without capsaicin) were taken in 20 patients with chronic neuropathic pain recruited from an independent pain clinic.
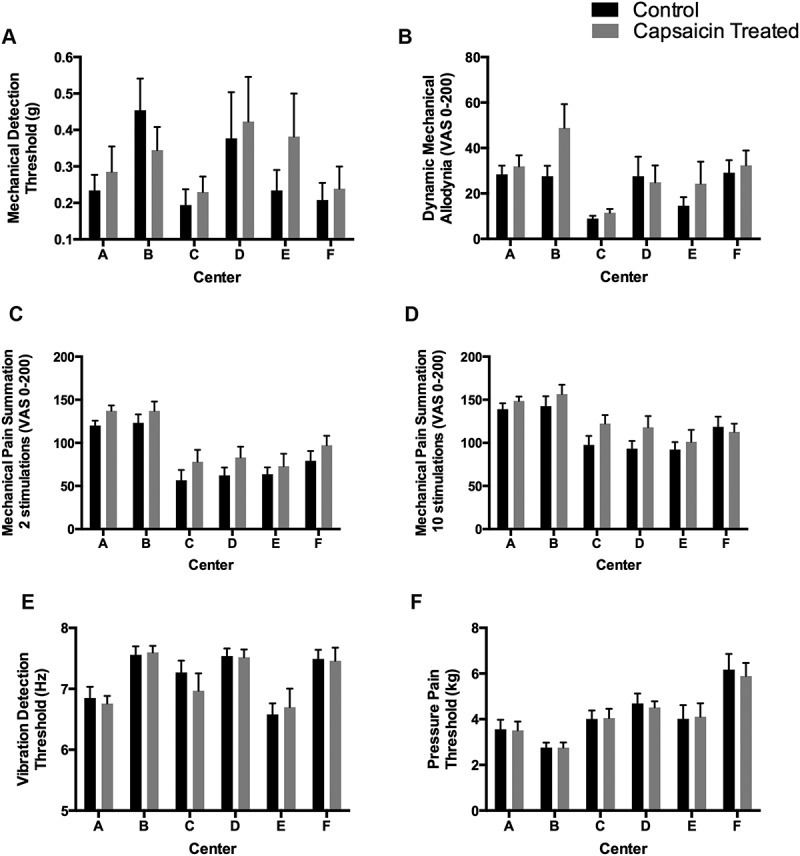
Results: Results revealed that six parameters detected a significant difference between the capsaicin-treated and the control skin areas: (1) cold detection threshold (CDT) and (2) cold pain threshold (CPT) are lower on the capsaicin-treated side, indicating a decreased in cold sensitivity; (3) heat pain threshold (HPT) was lower on the capsaicin-treated side in healthy subjects, suggesting an increased heat pain sensitivity; (4) dynamic mechanical allodynia (DMA); (5) mechanical pain after two stimulations (MPS2); and (6) mechanical pain summation after ten stimulations (MPS10), are increased on the capsaicin-treated side, suggesting an increased in mechanical pain (P < 0.002). CDT, CPT and HPT showed comparable effects across all six centers, with CPT and HPT demonstrating the best sensitivity. Data from the patients showed significant difference between affected and unaffected body side but only with CDT.
Conclusion: These results provide further support for the application of QST in multicenter studies examining normal and pathological pain responses.
Contexte: L’utilisation de tests sensoriels quantitatifs (QST) dans les études multicentriques est limitée, en partie à cause de l’absence de procédures normalisées au sein des centres.But: évaluer l’application du modèle de la douleur traitée par capsaïcine en tant que modèle expérimental humain de substitution pour la douleur neuropathique dans différents centres et vérifier les variations dans les mesures des tests sensoriels quantitatifs entre les centres.Méthodes: Une étude multicentrique menée par le Réseau québécois de recherche sur la douleur dans six laboratoires a permis d’évaluer neuf paramètres de tests sensoriels quantitatifs chez 60 sujets en bonne santé traités par capsaïcine topique afin de modéliser la douleur unilatérale et l’allodynie. Les mêmes mesures (sans capsaïcine) ont été prises chez 20 patients atteints de douleur neuropathique chronique recrutés dans une clinique de la douleur indépendante.Résultats: Les résultats ont révélé une différence significative entre la zone de peau traitée à la capsaïcine et la zone contrôle pour six paramètres : 1) le seuil de détection du froid (CTF) et 2) le seuil de perception de la douleur causée par le froid (CPT) étaient plus bas sur le côté traité par capsaïcine chez les sujets en bonne santé, ce qui indique une diminution de la sensibilité au froid, 3) Le seuil de perception de la douleur causée par la chaleur (HPT) était plus bas sur le côté traité par capsaïcine chez les sujets en bonne santé, ce qui suggère une augmentation de la sensibilité à la douleur causée par la chaleur; 4) l’allodynie mécanique dynamique (DMA), 5) la douleur mécanique après deux stimulations (MPS2) et 6) la somme de la douleur mécanique après 10 stimulations (MPS10) ont augmenté sur le côté traité à la capsaïne, ce qui suggère une augmentation de la douleur mécanique (p < 0,002). Le CDT, le CPT et le HPT ont démontré des effets comparables dans les six centres, le CPT et le HPT démontrant la meilleure sensibilité. Les données des patients ont révélé une différence significative entre le côté affecté et le non côté non affecté, mais seulement dans le cas du CDT.Conclusion: Ces résultats soutiennent l’application de tests sensoriels quantitatifs dans les études multicentriques portant sur les réponses normales et pathologiques à la douleur.
Keywords: multicenter study; neuropathic pain; quantitative sensory testing.
Published with license by Taylor & Francis Group, LLC.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures



References
-
- Geber C, Klein T, Azad S, Birklein F, Gierthmuhlen J, Huge V, Lauchart M, Nitzsche D, Stengel M, Valet M, et al. Test-retest and interobserver reliability of quantitative sensory testing according to the protocol of the German research network on neuropathic pain (DFNS): a multi-centre study. Pain. 2011;152(3):548–56. doi: 10.1016/j.pain.2010.11.013. - DOI - PubMed
-
- Rolke R, Baron R, Maier C, Tolle TR, Treede RD, Beyer A, Binder A, Birbaumer N, Birklein F, Botefur IC, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): standardized protocol and reference values. Pain. 2006;123(3):231–43. doi: 10.1016/j.pain.2006.01.041. - DOI - PubMed
-
- Kemler MA, Schouten HJ, Gracely RH.. Diagnosing sensory abnormalities with either normal values or values from contralateral skin: comparison of two approaches in complex regional pain syndrome I. Anesthesiology. 2000;93:718–27. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases