

Shock Severity Assessment in Cardiac Intensive Care Unit Patients With Sepsis and Mixed Septic-Cardiogenic Shock
- PMID: 35005436
- PMCID: PMC8715298
- DOI: 10.1016/j.mayocpiqo.2021.11.008
Shock Severity Assessment in Cardiac Intensive Care Unit Patients With Sepsis and Mixed Septic-Cardiogenic Shock
Abstract
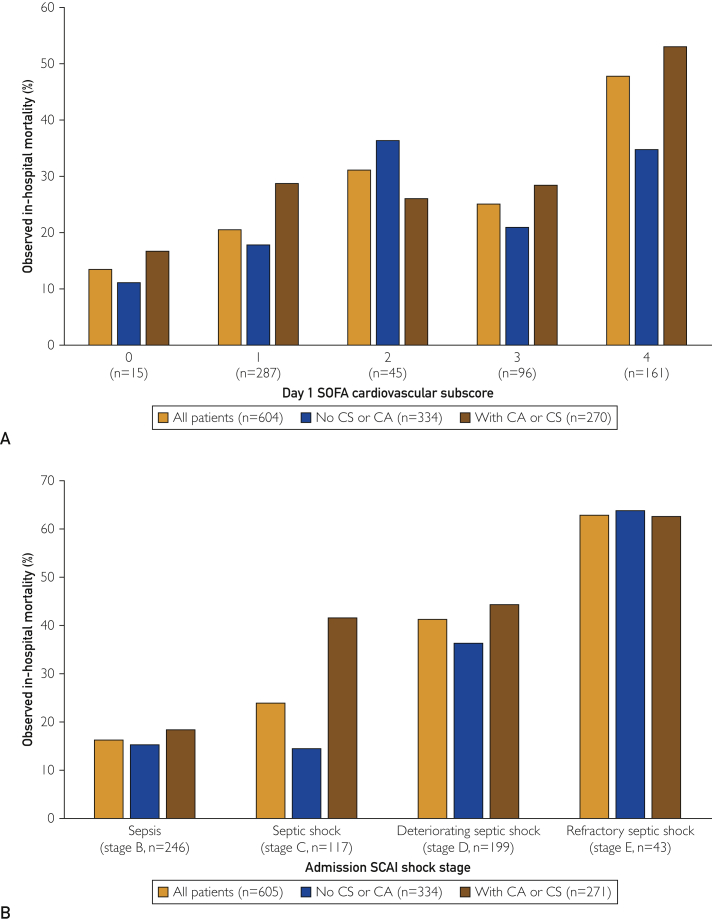
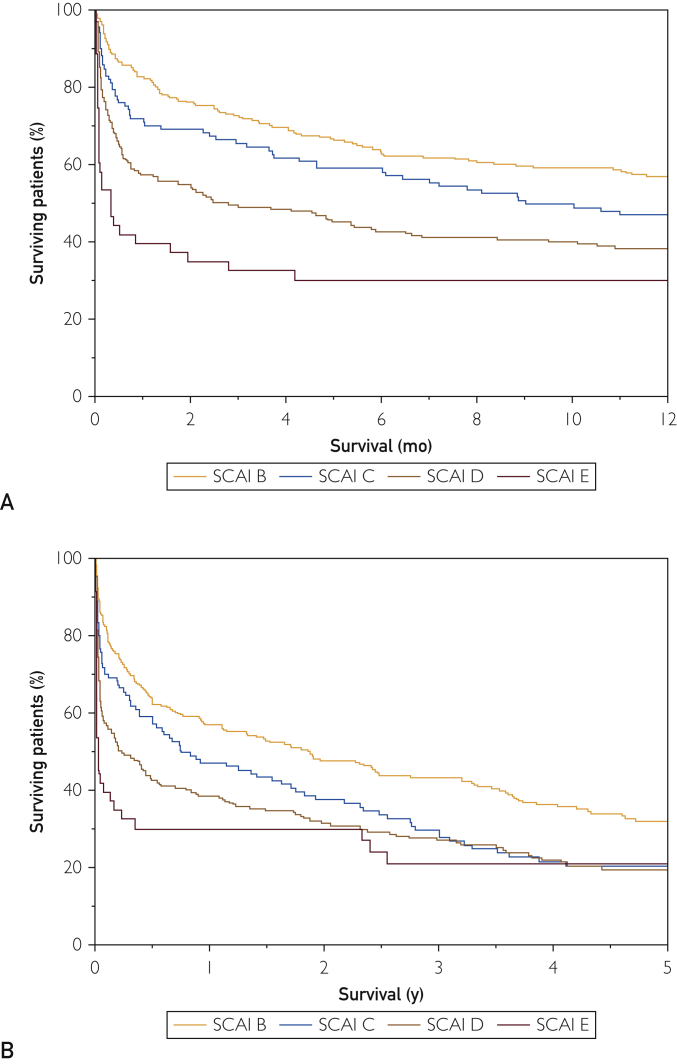
We sought to validate the Society for Cardiovascular Angiography and Interventions (SCAI) cardiogenic shock classification for mortality risk stratification in patients with sepsis and concomitant cardiovascular disease or mixed septic-cardiogenic shock. We conducted a single-center retropective cohort study of cardiac intensive care unit patients with an admission diagnosis of sepsis. We used clinical, vital sign, and laboratory data during the first 24 hours after admission to assign SCAI shock stage. We included 605 patients with a median age of 69.4 years (interquartile range, 57.9 to 79.8 years), 222 of whom (36.7%) were female. Acute coronary syndrome or heart failure was present in 480 patients (79.3%), and cardiogenic shock or cardiac arrest was present in 271 patients (44.8%). The median day 1 Sequential Organ Failure Assessment (SOFA) cardiovascular subscore was 1.5 (interquartile range, 1 to 4), and the admission SCAI shock stage distribution was stage B, 40.7% (246); stage C, 19.3% (117); stage D, 32.9% (199); and stage E, 7.1% (43). In-hospital mortality occurred in 177 of the 605 patients (29.3%) and increased incrementally with higher SCAI shock stage. After multivariable adjustment, admission SCAI shock stage was associated with in-hospital mortality (adjusted odds ratio per stage, 1.46; 95% CI, 1.14 to 1.88; P=.003). Admission SCAI shock stage had higher discrimination for in-hospital mortality than the day 1 SOFA cardiovascular subscore (area under the receiver operating characteristic curve, 0.68 vs 0.64; P=.04 by the DeLong test). Admission SCAI shock stage was associated with 1-year mortality (adjusted hazard ratio per stage, 1.19; 95% CI, 1.03 to 1.37; P=.02). The SCAI shock classification provides improved mortality risk stratification over the day 1 SOFA cardiovascular subscore in cardiac intensive care unit patients with sepsis and concomitant cardiovascular disease or mixed septic-cardiogenic shock.
Keywords: APACHE, Acute Physiology and Chronic Health Evaluation; AUC, area under the receiver operating characteristic curve; CICU, cardiac intensive care unit; CS, cardiogenic shock; OR, odds ratio; SCAI, Society for Cardiovascular Angiography and Interventions; SIRS, systemic inflammatory response syndrome; SOFA, Sequential Organ Failure Assessment.
© 2021 The Authors.
Figures
Similar articles
-
Serial Assessment of Shock Severity in Cardiac Intensive Care Unit Patients.J Am Heart Assoc. 2023 Dec 5;12(23):e032748. doi: 10.1161/JAHA.123.032748. Epub 2023 Nov 28. J Am Heart Assoc. 2023. PMID: 37930059 Free PMC article.
-
Cardiogenic Shock Classification to Predict Mortality in the Cardiac Intensive Care Unit.J Am Coll Cardiol. 2019 Oct 29;74(17):2117-2128. doi: 10.1016/j.jacc.2019.07.077. Epub 2019 Sep 20. J Am Coll Cardiol. 2019. PMID: 31548097
-
Systemic Inflammatory Response Syndrome Is Associated With Increased Mortality Across the Spectrum of Shock Severity in Cardiac Intensive Care Patients.Circ Cardiovasc Qual Outcomes. 2020 Dec;13(12):e006956. doi: 10.1161/CIRCOUTCOMES.120.006956. Epub 2020 Dec 7. Circ Cardiovasc Qual Outcomes. 2020. PMID: 33280435
-
Cardiogenic Shock Classification and Associated Mortality Risk.Mayo Clin Proc. 2023 May;98(5):771-783. doi: 10.1016/j.mayocp.2022.12.007. Epub 2023 Apr 5. Mayo Clin Proc. 2023. PMID: 37028976 Review.
-
Time from Admission to Right Heart Catheterization in Cardiogenic Shock Patients.Curr Probl Cardiol. 2023 Feb;48(2):101441. doi: 10.1016/j.cpcardiol.2022.101441. Epub 2022 Oct 8. Curr Probl Cardiol. 2023. PMID: 36216201 Review.
Cited by
-
Validation of SCAI Shock Staging in Critically Ill Medical Intensive Care Unit Patients With Sepsis and Septic Shock.J Community Hosp Intern Med Perspect. 2025 Jan 6;15(1):13-21. doi: 10.55729/2000-9666.1436. eCollection 2025. J Community Hosp Intern Med Perspect. 2025. PMID: 39867142 Free PMC article.
-
Advances in the Staging and Phenotyping of Cardiogenic Shock: Part 1 of 2.JACC Adv. 2022 Oct 28;1(4):100120. doi: 10.1016/j.jacadv.2022.100120. eCollection 2022 Oct. JACC Adv. 2022. PMID: 38939719 Free PMC article. Review.
-
Myocardial Infarction-Associated Shock: A Comprehensive Analysis of Phenotypes, SCAI Classification, and Outcome Assessment.Medicina (Kaunas). 2025 Jan 13;61(1):103. doi: 10.3390/medicina61010103. Medicina (Kaunas). 2025. PMID: 39859085 Free PMC article.
-
Application of the SCAI classification to admission of patients with cardiogenic shock: Analysis of a tertiary care center in a middle-income country.PLoS One. 2022 Aug 16;17(8):e0273086. doi: 10.1371/journal.pone.0273086. eCollection 2022. PLoS One. 2022. PMID: 35972946 Free PMC article.
-
Survival prediction for heart failure complicated by sepsis: based on machine learning methods.Front Med (Lausanne). 2024 Oct 3;11:1410702. doi: 10.3389/fmed.2024.1410702. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39421876 Free PMC article.
References
-
- Jentzer J.C., Ahmed A.M., Vallabhajosyula S., et al. Shock in the cardiac intensive care unit: changes in epidemiology and prognosis over time. Am Heart J. 2021;232:94–104. - PubMed
-
- Jentzer J.C., van Diepen S., Barsness G.W., et al. Changes in comorbidities, diagnoses, therapies and outcomes in a contemporary cardiac intensive care unit population. Am Heart J. 2019;215:12–19. - PubMed
-
- Jentzer J.C., Lawler P.R., van Diepen S., et al. Systemic inflammatory response syndrome is associated with increased mortality across the spectrum of shock severity in cardiac intensive care patients. Circ Cardiovasc Qual Outcomes. 2020;13(12) - PubMed
-
- Jentzer J.C., Wiley B., Bennett C., et al. Temporal trends and clinical outcomes associated with vasopressor and inotrope use in the cardiac intensive care unit. Shock. 2020;53(4):452–459. - PubMed
LinkOut - more resources
Full Text Sources
