

Sacral anatomical parameters varies in different Roussouly sagittal shapes as well as their relations to lumbopelvic parameters
- PMID: 35005446
- PMCID: PMC8717110
- DOI: 10.1002/jsp2.1180
Sacral anatomical parameters varies in different Roussouly sagittal shapes as well as their relations to lumbopelvic parameters
Abstract
Purpose: To study the normal variations in sacral anatomical parameters in different Roussouly sagittal shapes and the association between sacral anatomical parameters and lumbopelvic parameters in healthy adults.
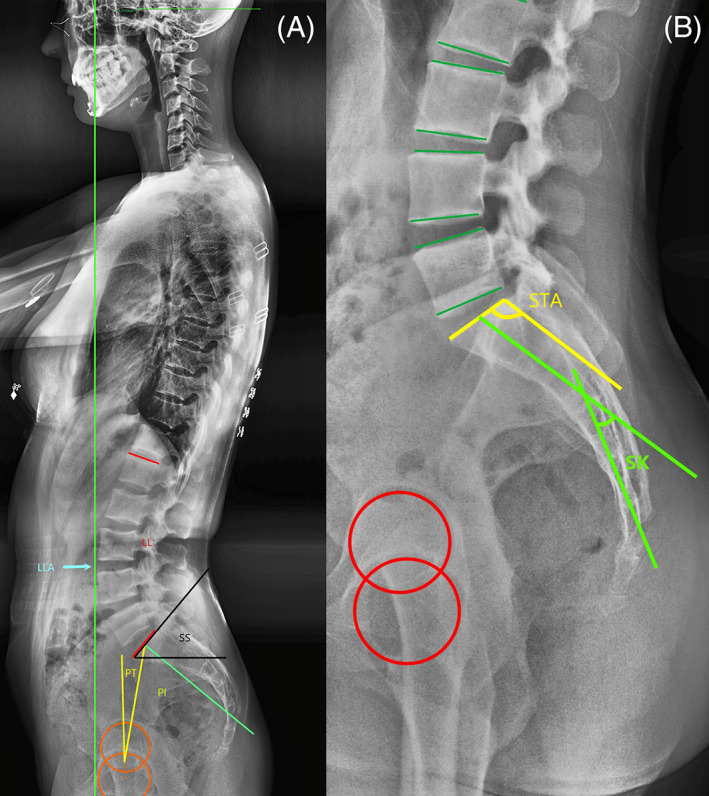
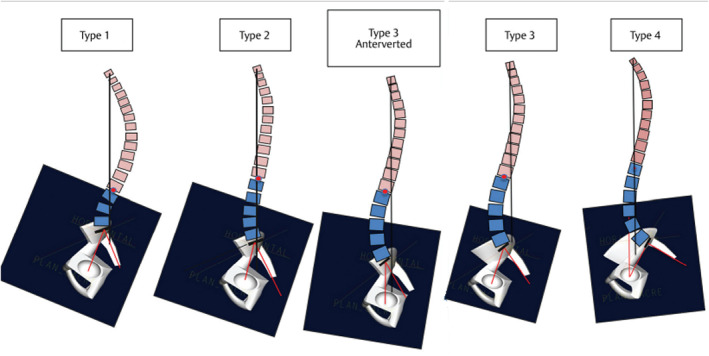
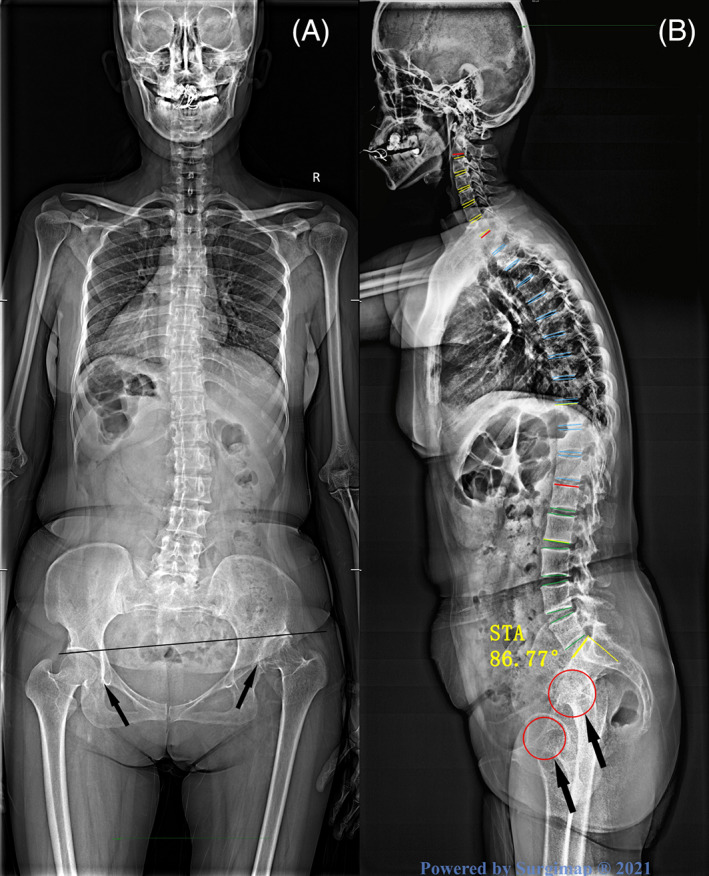
Methods: A cohort of 239 healthy volunteers between 18 and 45 years old was enrolled in this study. A full-spine, standing X-ray was taken for each volunteer. The following parameters were measured: the sacral table angle (STA), sacral kyphosis (SK), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), and lumbar lordosis apex (LLA). Two hundred and thirty-nine volunteers were classified into five groups according to the Roussouly classification. The differences in sagittal parameters among the five groups were evaluated by one-way analysis of variance. The correlations between lumbopelvic parameters and sacral anatomical parameters were analyzed, and simple linear regressions were simultaneously constructed.
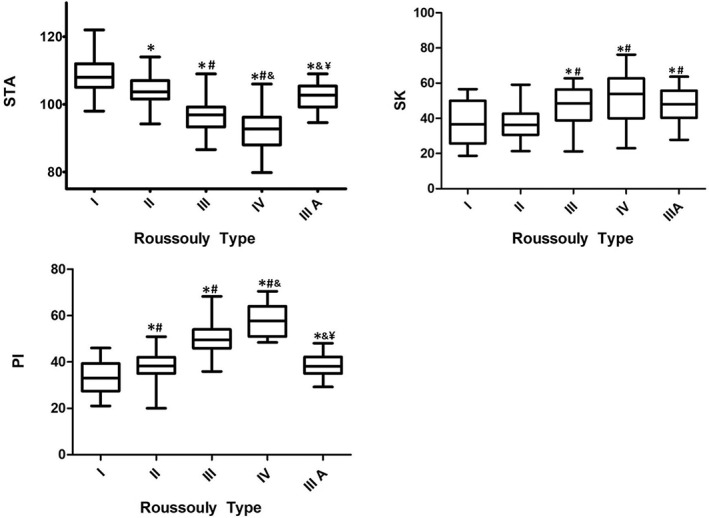
Result: The sacral anatomical parameters vary in different Roussouly sagittal shapes. Correlation analysis revealed that the significant correlations between sacral anatomical parameters and lumbopelvic parameters. The STA correlated with PI (r = -.690, P <.001), PT (r = -.216, P = .001), SS (r = -.631, P <.001), LL (r = -.491, P <.001), and LLA (r = 0.515, P <.001). The corresponding regression formulae were as follows: PI = -0.991*STA + 143(R 2 = .476), LL = 0.870*STA-135.1(R 2 = .242), and LLA = 0.039*STA -0.087(R 2 = .265). The SK correlated with PI (r = .471, P <.001), PT (r = .445, P = .001), SS (r = .533, P <.001), LL (r = .438, P <.001), and the LLA (r = -.265, P <.001). The corresponding regression formulae were as follows: PI = 0.38*SK + 27.22(R 2 = .396), LL = -0.35*SK - 35.99(R 2 = .192), and LLA = -0.01*SK + 4.25(R 2 = .201).
Conclusions: The sacral anatomical parameters vary in different Roussouly sagittal shapes and have strong correlations with lumbopelvic parameters, which demonstrates that the specific lumbar shape can be affected by the sacral morphology. Moreover, the predictive models of lumbopelvic parameters based on SK and STA have been provided, which demonstrates constant sacral anatomical parameters could serve as good supplementary index of PI to predict ideal lumbar parameters.
Keywords: Roussouly classification; lumbopelvic parameters; predictive models; sacral anatomical parameters; sacral kyphosis; sacral table angle.
© 2021 The Authors. JOR Spine published by Wiley Periodicals LLC on behalf of Orthopaedic Research Society.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Vialle R, Levassor N, Rillardon L, et al. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87(2):260‐267. - PubMed
-
- Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005;18(1):40‐47. - PubMed
-
- Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine. 2005;30(3):346‐353. - PubMed
-
- During J, Goudfrooij H, Keessen W, et al. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine. 1985;10(1):83‐87. - PubMed
-
- Laouissat F, Sebaaly A, Gehrchen M, Roussouly P. Classification of normal sagittal spine alignment: refounding the Roussouly classification. Eur Spine J. 2018;27(8):2002‐2011. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
