

The impact of specialised treatment of low back pain on health care costs and productivity in a nationwide cohort
- PMID: 35005584
- PMCID: PMC8718977
- DOI: 10.1016/j.eclinm.2021.101247
The impact of specialised treatment of low back pain on health care costs and productivity in a nationwide cohort
Abstract
Background: Low back pain (LBP) is the most common diagnosis responsible for sick leave, long-term disability payments, and early retirements. Studies have suggested that the relatively small proportion of patients referred to a specialist for treatment, either conservative or surgical, accounts for most of the total costs of back pain. However, a complete and long-term picture of the socioeconomic burden associated with these two treatment regimens is lacking.
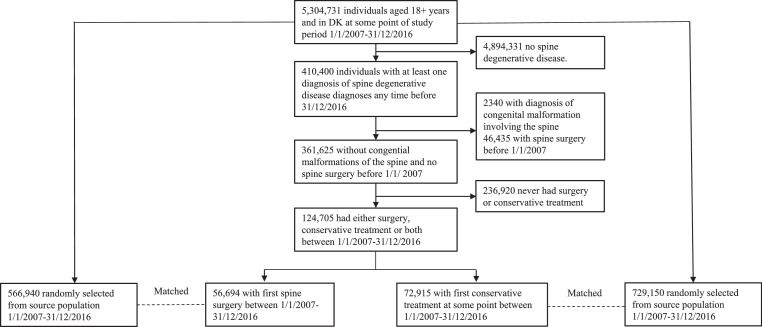
Methods: From a cohort encompassing the entire population in Denmark (5.8 million inhabitants), we identified patients with LBP referred to specialised treatment, either conservative or surgical, during 2007-2016. According to treatment modality, two different cohorts were constructed. Each patient was matched with ten background population controls based on age, sex, region of residency and time of treatment (month and year). Using extensive, nationwide register data, the healthcare costs and loss of productivity from two years before the first intervention until 2018 was investigated.
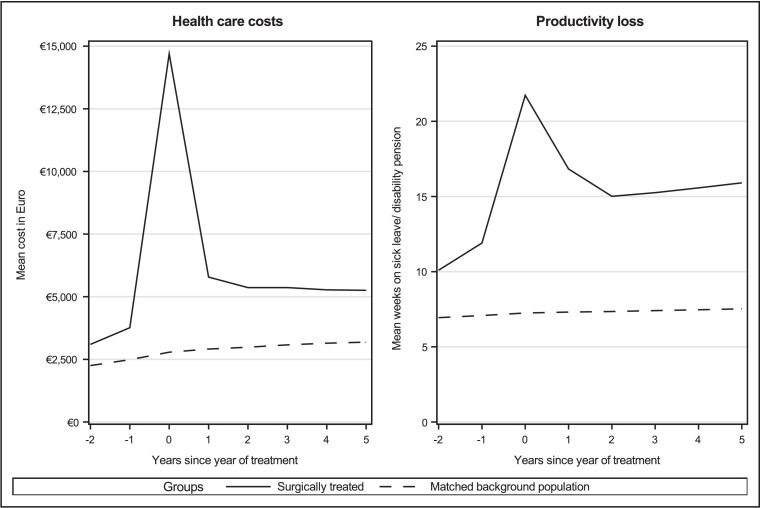
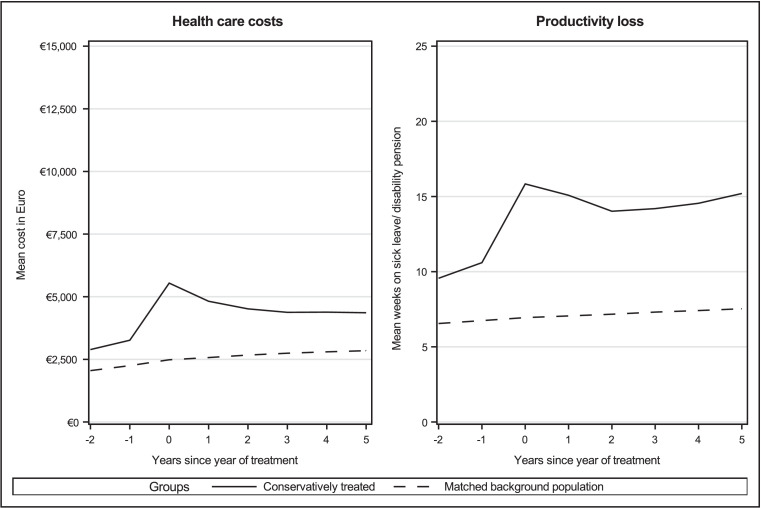
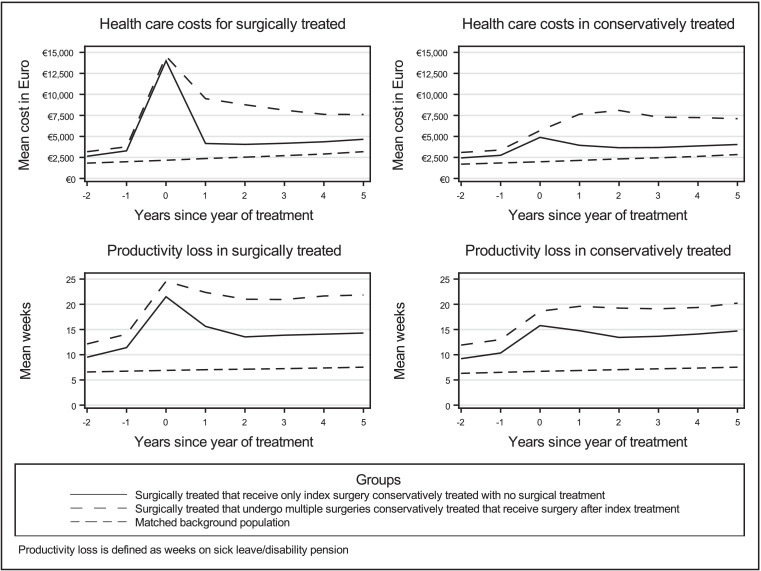
Findings: A total of 56,694 patients underwent surgical treatment, and 72,915 patients conservative treatment. Both cohorts had a significantly higher baseline cost two years before treatment compared with the background population controls. These measures increased sharply during the year after treatment. Five years after treatment, healthcare costs and loss of productivity remained proportionally similarly increased for the two treatment groups compared to the background population. Multiple surgeries had detrimental effects on long term productivity for the patients, and spouses to patients had marginally increased loss of productivity.
Interpretation: The results show that patients referred to specialised treatment of LBP display poor socioeconomic prognosis, regardless of conservative or surgical treatment modality. This development was reinforced in patients undergoing multiple surgeries and was also observed among spouses to the patients. Our findings of substantial loss of productivity across subgroups indicate that measures of successful treatment need to be more nuanced.
Keywords: Low Back Pain; Socioeconomic; cost of illness; nationwide cohort.
© 2021 The Author(s).
Conflict of interest statement
SS received funding from Helsefonden, Aase and Ejner Danielsens Fond for his PhD, for which this paper is included. The funds were for data collection, salary for primary investigator and statistical analysis. Both where not for profit affiliations and neither had any involvement in the study and there was therefore no conflict of interests. The other authors declare no conflict of interests.
Figures
References
-
- Hartvigsen J., Hancock M.J., Kongsted A., et al. What low back pain is and why we need to pay attention. Lancet. 2018;391:2356–2367. - PubMed
-
- van Tulder M., Koes B., Bombardier C. Low back pain. Best Pract Res Clin Rheumatol. 2002;16:761–775. - PubMed
-
- Andersson G.B. Epidemiological features of chronic low-back pain. Lancet. 1999;354:581–585. - PubMed
-
- Deyo R.A., Weinstein J.N. Low back pain. N Engl J Med. 2001;344:363–370. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
