

Turmeric extract alleviates endocrine-metabolic disturbances in letrozole-induced PCOS by increasing adiponectin circulation: A comparison with Metformin
- PMID: 35005596
- PMCID: PMC8717583
- DOI: 10.1016/j.metop.2021.100160
Turmeric extract alleviates endocrine-metabolic disturbances in letrozole-induced PCOS by increasing adiponectin circulation: A comparison with Metformin
Erratum in
-
Erratum regarding previously published articles.Metabol Open. 2023 Jan 21;17:100231. doi: 10.1016/j.metop.2023.100231. eCollection 2023 Mar. Metabol Open. 2023. PMID: 36992679 Free PMC article.
Abstract
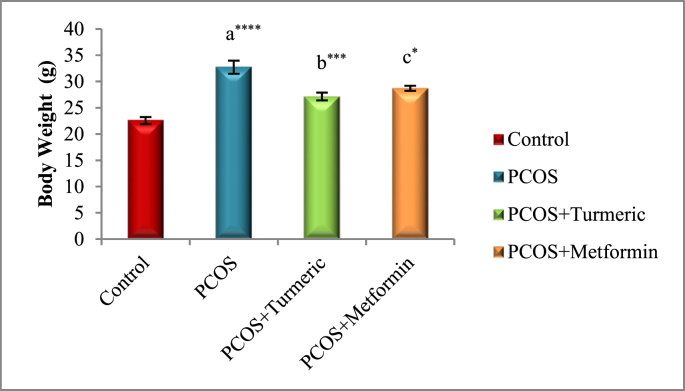
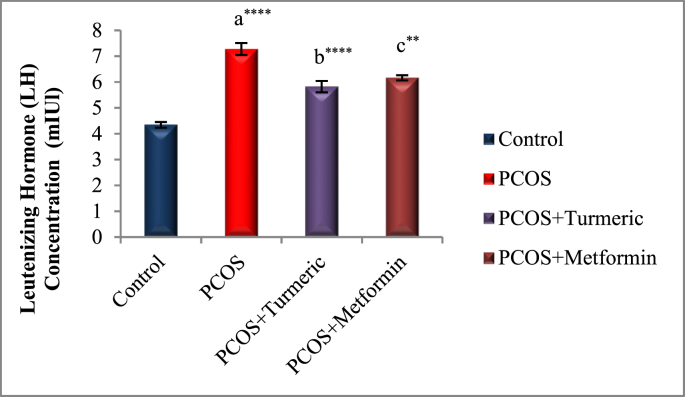
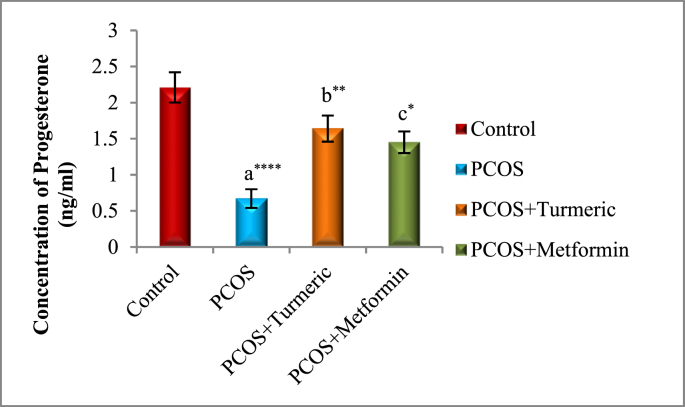
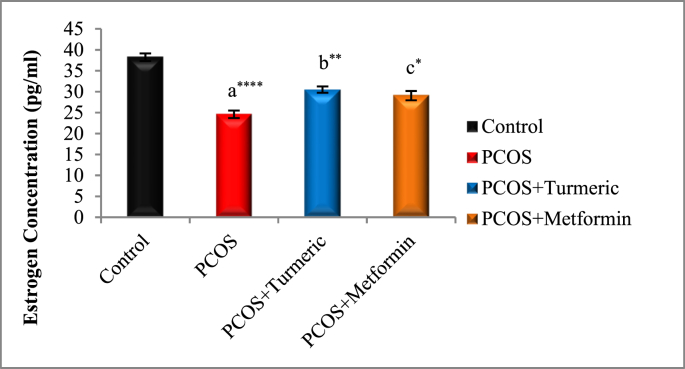
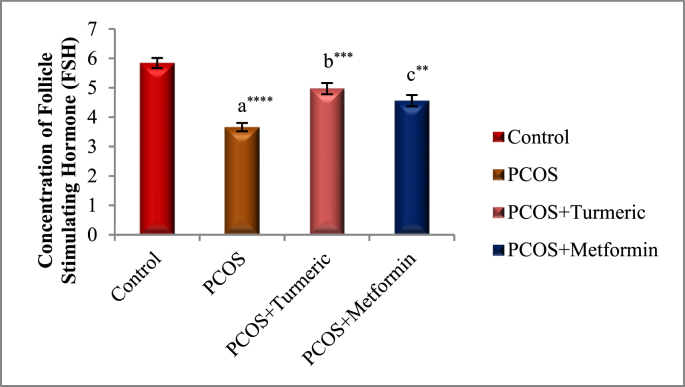
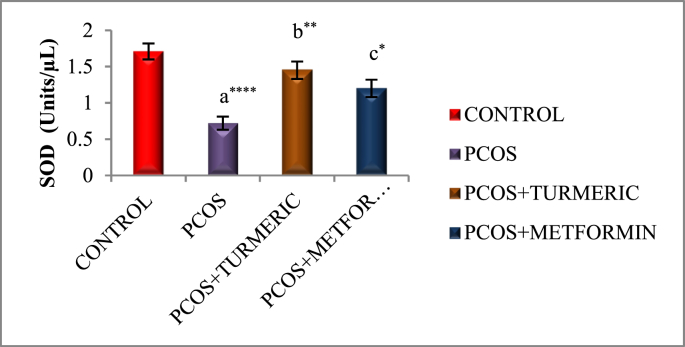
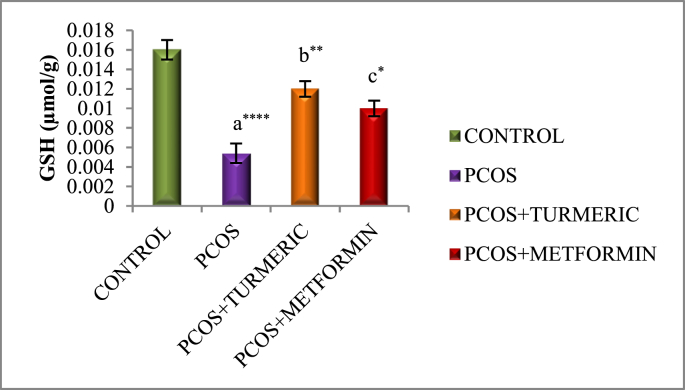
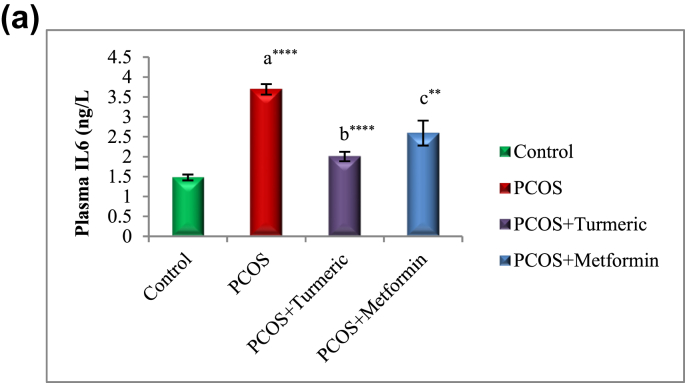
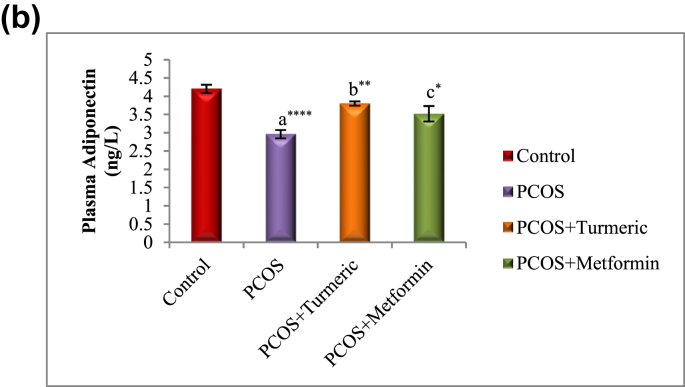
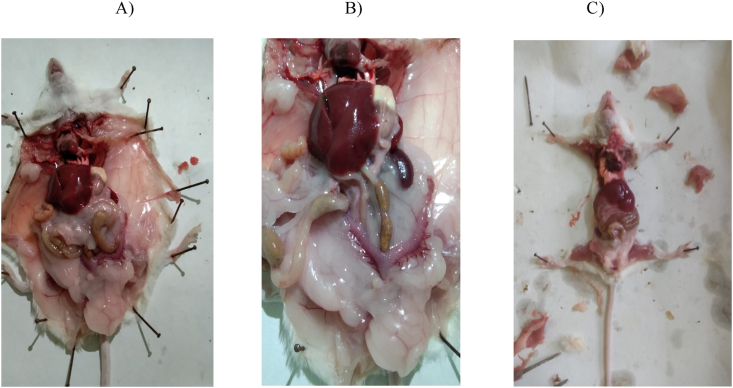
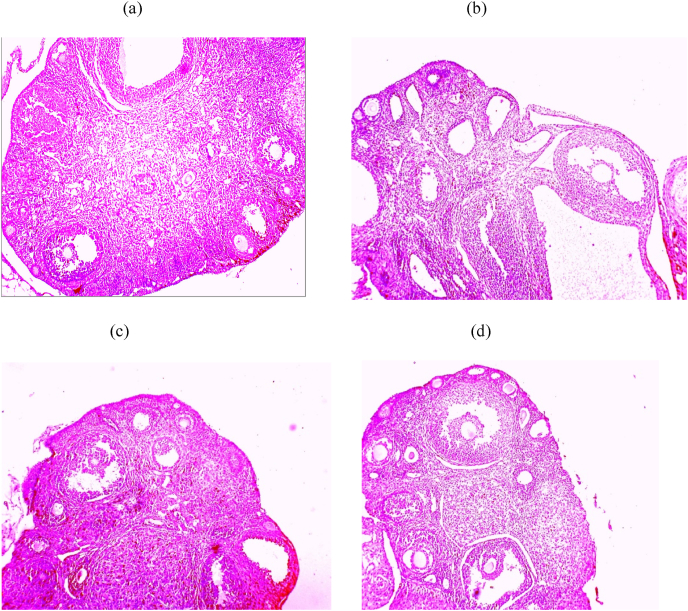
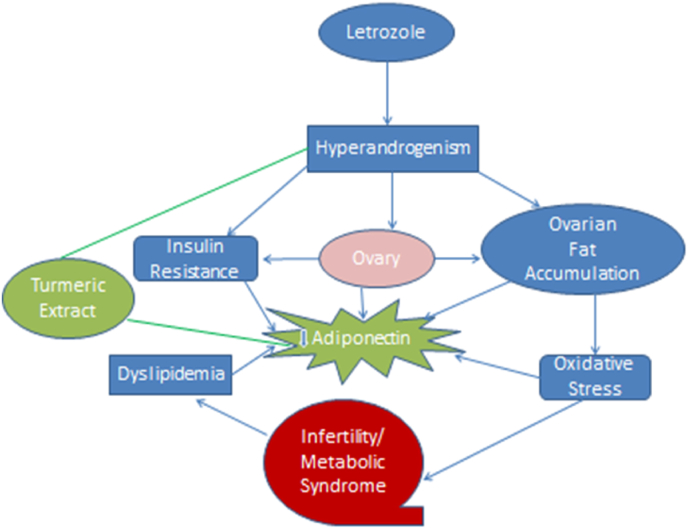
One of the most common causes of female infertility is polycystic ovarian syndrome, which affects 6-21% of the population. Regrettably, the currently available treatments are mostly symptomatic and ineffective. As a result, safer options are needed now more than ever. In a letrozole PCOS albino mouse model, the current study compares the therapeutic advantages of Turmeric extract (Curcuma longa) to metformin. Adiponectin is a circulating protein generated by adipocytes that has been linked to metabolic diseases (MDs) in an inverse relationship. The effects of Turmeric Extract (Curcuma Longa) in contrast to Metformin, as well as the involvement of adiponectin in endocrine-metabolic abnormalities in experimentally induced PCOS mice model, were studied in this study. Letrozole (6 mg/kg) was administered orally (p.o) for 21 days to induce PCOS, followed by a dose of Turmeric Extract (Curcuma longa) (175 mg/kg and p.o) and Metformin (150 mg/kg) for 30 days, both with normal saline water (0.9%) as the carrier. The findings revealed that LET-treated mice displayed PCOS-like characteristics, such as higher LH levels, increased body weight growth, and ovarian morphology with numerous cysts, increase in fasting blood glucose, lipid profile, plasma lipid peroxidation (MDA) and IL-6, as well as a decrease in serum Progesterone, Estrogen, FSH, SOD and GSH levels in the ovary. These changes were linked to lower levels of circulating adiponectin and were reversed when treated Turmeric extract. By altering circulating androgen-adiponectin balance, the data implies that Turmeric extract alleviates endocrine-metabolic abnormalities and inflammation-related comorbidities associated with LET-induced PCOS.
Keywords: Adiponectin; Metformin; Oxidative stress; Polycystic ovary syndrome; Turmeric extract (Curcuma Longa).
© 2021 The Author(s).
Figures

References
-
- Zafar U., Memon Z., Moin K., Agha S., Hassan J.A., Zehra D. Prevalence of PCOS with associated symptoms and complications at tertiary care hospital of Karachi. J Adv Med Med Res. 2019;30(4):1–9. doi: 10.9734/jammr/2019/v30i430190. - DOI
-
- Joham A.E., Teede H.J., Ranasinha S., Zoungas S., Boyle J. Prevalence of infertility and use of fertility treatment in women with Polycystic Ovary Syndrome: data from a large community-based cohort study. J Womens Health (Larchmt) 2015 Apr;24(4):299–307. doi: 10.1089/jwh.2014.5000. Epub 2015 Feb 5. PMID: 25654626. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
