

Systematic review and meta-analysis of COVID-19 maternal and neonatal clinical features and pregnancy outcomes up to June 3, 2021
- PMID: 35005663
- PMCID: PMC8720679
- DOI: 10.1016/j.xagr.2021.100049
Systematic review and meta-analysis of COVID-19 maternal and neonatal clinical features and pregnancy outcomes up to June 3, 2021
Abstract
Objective: COVID-19 is a rapidly changing and developing emergency that requires constant re-evaluation of available data. We report a systematic review and meta-analysis based on all published high-quality data up to and including June 3, 2021 on the maternal and neonatal outcomes in pregnant women infected with COVID-19.
Data sources: PubMed, SCOPUS, MEDLINE, ClinicalTrials.gov, and Web of Science databases were queried from inception up to June 3, 2021.
Study eligibility criteria: We included all clinical studies (prospective and retrospective cohort studies, case-control studies, case series, and rapid communications) that reported data on any maternal and neonatal outcomes of pregnant women with COVID-19.
Methods: The data were analyzed as pooled proportions or odds ratios and 95% confidence intervals in meta-analysis models.
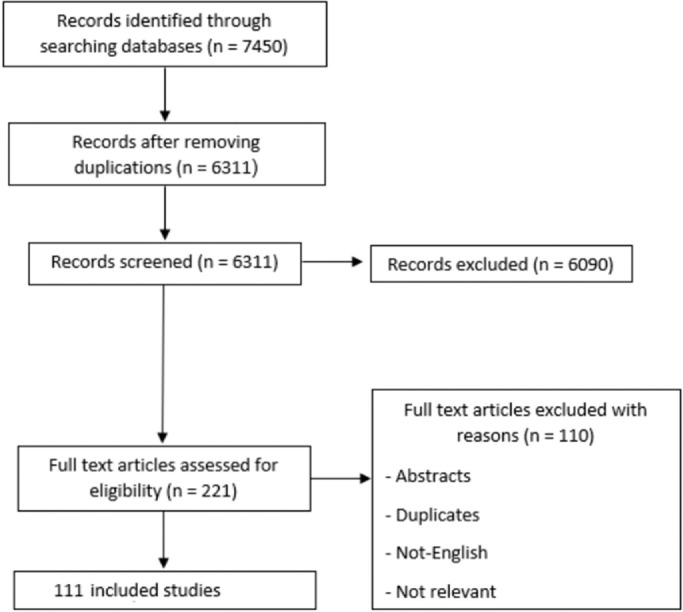
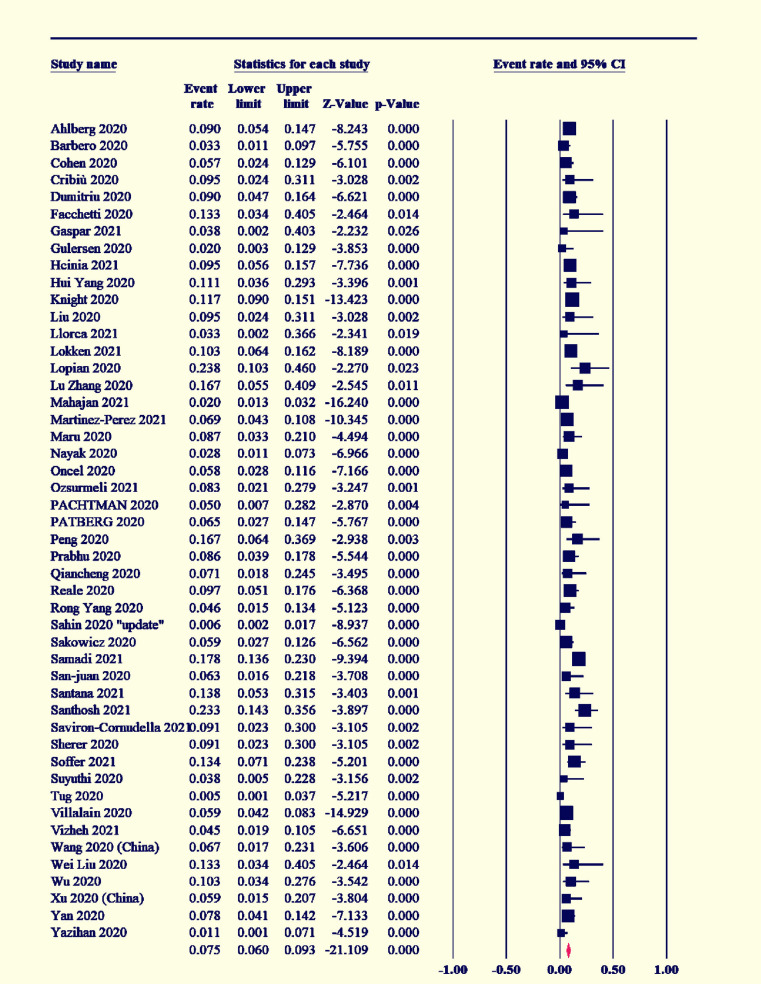
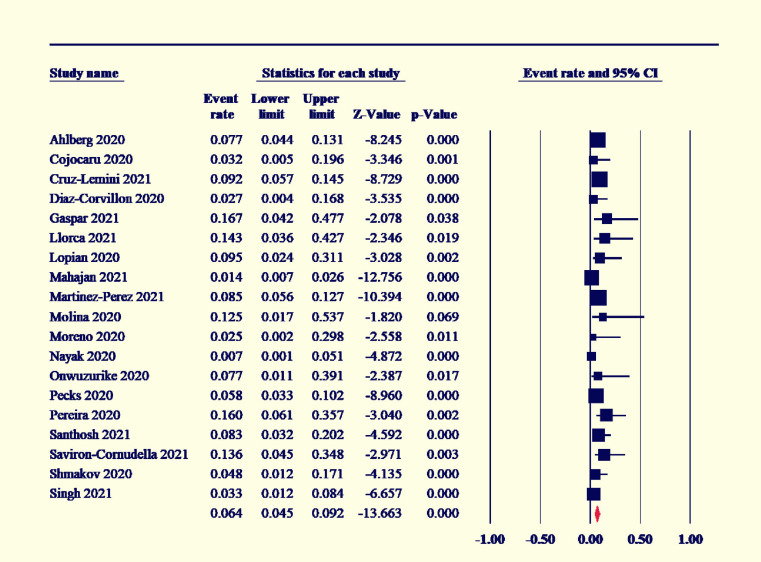
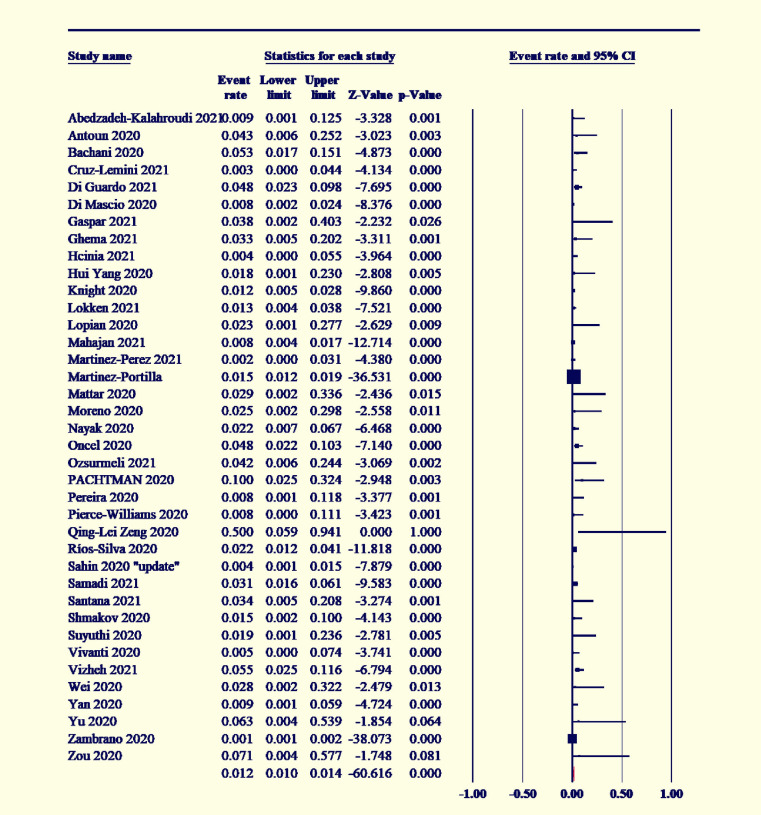
Results: We included 111 studies enrolling 42,754 COVID-19-positive pregnant women. From COVID-19-positive pregnant women, the incidence rates were 53.2% (95% confidence interval, 48-58.4) for cesarean delivery, 41.5% (95% confidence interval, 36.3-46.8) for spontaneous vaginal delivery, and 6.4% (95% confidence interval, 4.5-9.2) for operative delivery. The rates of some adverse neonatal events, including premature delivery (16.7%; 95% confidence interval, 12.8-21.5) and low birthweight (16.7%; 95% confidence interval, 12.8-21.5) were relatively high in mothers infected with COVID-19. Vertical transmission (3.5%; 95% confidence interval, 2.7-4.7), neonatal death (3%; 95% confidence interval, 2-4), stillbirth (1.9%; 95% confidence interval, 1.5-2.4), and maternal mortality (0.012%; 95% confidence interval, 0.010-0.014) were rare adverse events. The mean birthweight was 3069.7 g (95% confidence interval, 3009.7-3129.8 g). In the comparative analysis, COVID-19 significantly increased the risk of premature delivery (odds ratio, 1. 48 [95% confidence interval, 1.22-1.8]), preeclampsia (odds ratio, 1.6 [95% confidence interval, 1.2-2.1]), stillbirth (odds ratio, 2.36 [95% confidence interval, 1.24-4.462]), neonatal mortality (odds ratio, 3.35 [95% confidence interval, 1.07-10.5]), and maternal mortality (odds ratio, 3.08 [95% confidence interval, 1.5-6.3]). The pooled analyses were homogenous, with mild heterogeneity in premature delivery and preeclampsia outcomes.
Conclusion: The data must be interpreted with caution as limited data are available, and no complete assessment of bias is possible at this time. Our data suggest that pregnant women who test positive for COVID-19 seem to be at a higher risk of lower birth weights and premature delivery. There is no evidence at this time of the sharply increased maternal mortality that was seen previously with both the 2003 SARS and 2012 MERS pandemics.
Keywords: COVID-19 in pregnancy; COVID-19 pregnancy outcomes; SARS-CoV-2; coronavirus; pregnancy outcomes.
© 2022 The Authors.
Figures

References
-
- Getahun D, Ananth CV, Peltier MR, Smulian JC, Vintzileos AM. Acute and chronic respiratory diseases in pregnancy: associations with placental abruption. Am J Obstet Gynecol. 2006;195:1180–1184. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
