

Predicting 30-day return hospital admissions in patients with COVID-19 discharged from the emergency department: A national retrospective cohort study
- PMID: 35005705
- PMCID: PMC8716570
- DOI: 10.1002/emp2.12595
Predicting 30-day return hospital admissions in patients with COVID-19 discharged from the emergency department: A national retrospective cohort study
Abstract
Objectives: Identification of patients with coronavirus disease 2019 (COVID-19) at risk for deterioration after discharge from the emergency department (ED) remains a clinical challenge. Our objective was to develop a prediction model that identifies patients with COVID-19 at risk for return and hospital admission within 30 days of ED discharge.
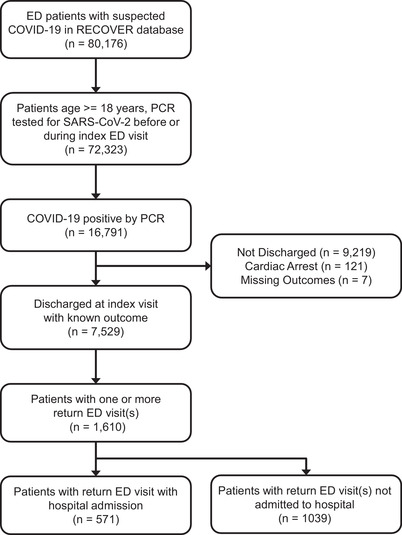
Methods: We performed a retrospective cohort study of discharged adult ED patients (n = 7529) with SARS-CoV-2 infection from 116 unique hospitals contributing to the National Registry of Suspected COVID-19 in Emergency Care. The primary outcome was return hospital admission within 30 days. Models were developed using classification and regression tree (CART), gradient boosted machine (GBM), random forest (RF), and least absolute shrinkage and selection (LASSO) approaches.
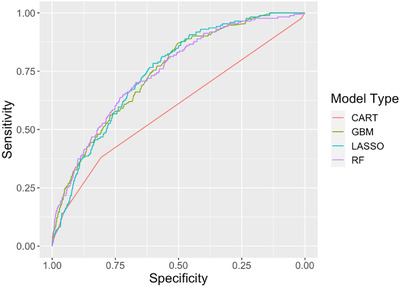
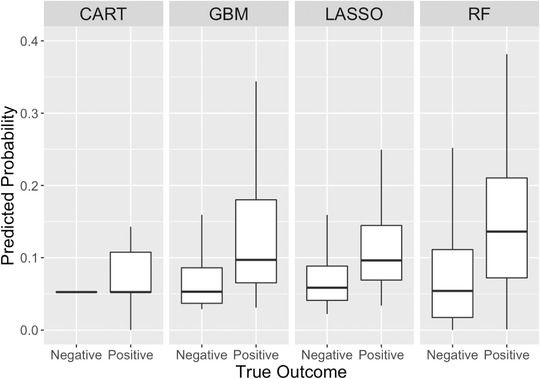
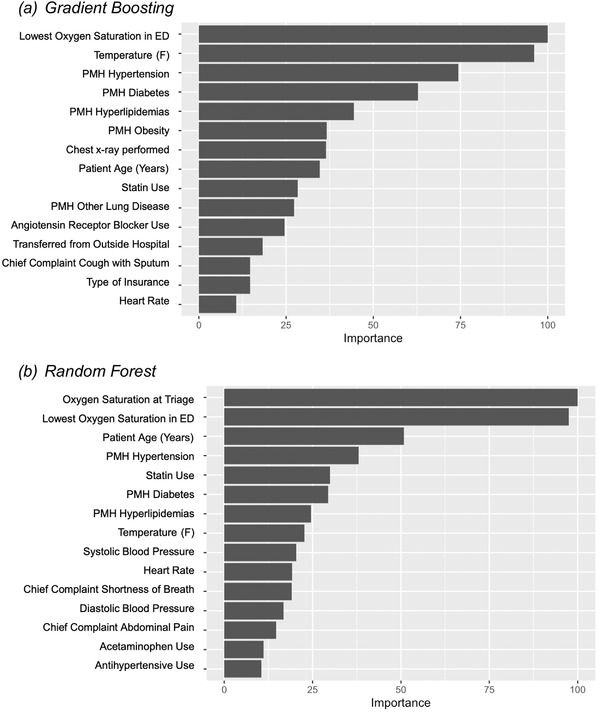
Results: Among patients with COVID-19 discharged from the ED on their index encounter, 571 (7.6%) returned for hospital admission within 30 days. The machine-learning (ML) models (GBM, RF, and LASSO) performed similarly. The RF model yielded a test area under the receiver operating characteristic curve of 0.74 (95% confidence interval [CI], 0.71-0.78), with a sensitivity of 0.46 (95% CI, 0.39-0.54) and a specificity of 0.84 (95% CI, 0.82-0.85). Predictive variables, including lowest oxygen saturation, temperature, or history of hypertension, diabetes, hyperlipidemia, or obesity, were common to all ML models.
Conclusions: A predictive model identifying adult ED patients with COVID-19 at risk for return for return hospital admission within 30 days is feasible. Ensemble/boot-strapped classification methods (eg, GBM, RF, and LASSO) outperform the single-tree CART method. Future efforts may focus on the application of ML models in the hospital setting to optimize the allocation of follow-up resources.
Keywords: COVID‐19; SARS‐CoV‐2; clinical prediction model; discharge planning; emergency department; machine learning; prognosis; readmissions.
© 2021 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
Samuel A. McDonald declares grant funding as site coinvestigator for “Predictors of Severe COVID Outcomes” funded and sponsored by Verily Life Sciences, and the Innovative Support for Patients with SARS‐COV2 Infections Registry (INSPIRE) funded by the Centers for Disease Control and Prevention, “Modeling of Infectious Network Dynamics for Surveillance, Control and Prevention Enhancement (MINDSCAPE).”
Figures
References
-
- Centers for Disease Control and Prevention . COVID Data Tracker. Centers for Disease Control and Prevention; 2021.
-
- Wood F, Roe T, Newman J, Wood L. Risk factors for deterioration in mild COVID‐19 remain undefined. Emerg Med J. 2021;38(5):406. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
