

Rapid versus slow withdrawal of antiepileptic drugs
- PMID: 35005782
- PMCID: PMC8744136
- DOI: 10.1002/14651858.CD005003.pub4
Rapid versus slow withdrawal of antiepileptic drugs
Abstract
Background: The ideal objective of treating a person with epilepsy is to induce remission (free of seizures for some time) using antiepileptic drugs (AEDs) and withdraw the AEDs without causing seizure recurrence. Prolonged usage of AEDs may have long-term adverse effects. Hence, when a person with epilepsy is in remission, it is logical to attempt to discontinue the medication. The timing of withdrawal and the mode of withdrawal arise while contemplating withdrawal of AEDs. This review examines the evidence for the rate of withdrawal of AEDs (whether rapid or slow tapering) and its effect on seizure recurrence. This is an updated version of the Cochrane Review previously published in 2020.
Objectives: To quantify risk of seizure recurrence after rapid (tapering period of three months or less) or slow (tapering period of more than three months) discontinuation of antiepileptic drugs in adults and children with epilepsy who are in remission, and to assess which variables modify the risk of seizure recurrence.
Search methods: For the latest update, on 8 November 2021, we searched: Cochrane Register of Studies (CRS Web), MEDLINE (Ovid), and SCOPUS. There were no language restrictions. CRS Web includes randomized or quasi-randomized, controlled trials from PubMed, Embase, ClinicalTrials.gov, the World Health Organization International Clinical Trials Registry Platform (ICTRP), CENTRAL, and the Specialized Registers of Cochrane Review Groups including Epilepsy.
Selection criteria: Randomized controlled trials that evaluated withdrawal of AEDs in a rapid or slow tapering after varying periods of seizure control in people with epilepsy.
Data collection and analysis: Two review authors independently assessed the trials for inclusion and extracted the data. The outcomes assessed included seizure freedom after one, two, or five years of AED withdrawal; time to recurrence of seizure following withdrawal; occurrence of status epilepticus; mortality; morbidity due to seizure, such as injuries, fractures, and aspiration pneumonia; and quality of life (assessed by validated scale).
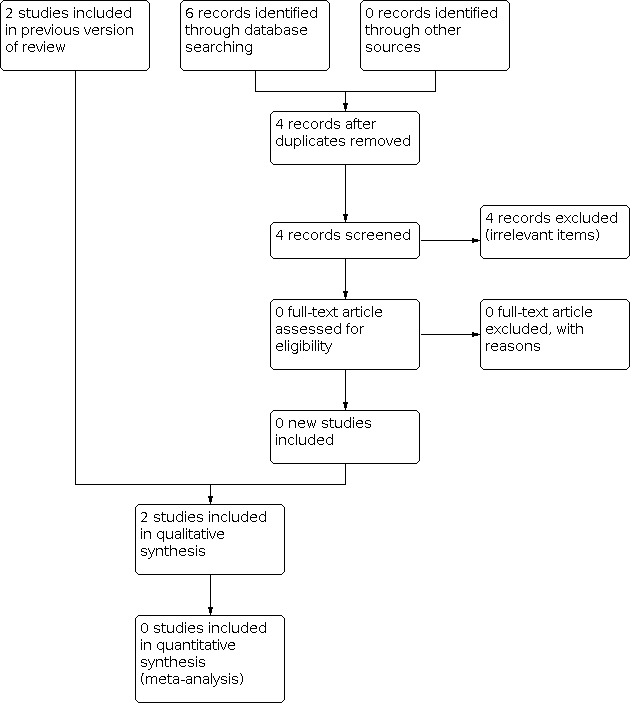
Main results: There are two included studies in this review. One study randomized 57 children with epilepsy with seizure freedom for at least two years to taper down the AED over one or six months. The study was not blinded and there were no details of randomization. Over the period of 54 months of follow-up, 20/30 participants in the one-month group remained seizure-free compared to 15/27 participants in the six-month group (no evidence of a difference). There was no information on time of seizure recurrence for each group to allow a comparison. The other study involved 149 children. There was a non-significant trend towards a lower risk of seizure recurrence after one year of AED withdrawal in participants allocated to slow tapering (risk ratio (RR) 0.76, 95% confidence interval (CI) 0.58 to 1.01; P = 0.06; very low-certainty evidence). At the end of two years, 30 participants were seizure free in the rapid-tapering group and 29 participants in the slow-tapering group (RR 0.87, 95% CI 0.58 to 1.29; P = 0.48; very low-certainty evidence). At the end of five years, 10 participants were seizure free in the rapid-tapering group and six participants in the slow-tapering group (RR 1.40, 95% CI 0.54 to 3.65; P = 0.49; very low-certainty evidence). There were no data for the other outcomes. Due to the methodological heterogeneity and the difference in the duration of tapering, we did not perform a quantitative synthesis of these studies. Currently, one Italian trial is ongoing that is investigating if a slow or a rapid withdrawal schedule of AEDs influences return of seizures (relapse) in adults with focal or generalized epilepsy who have been seizure free for at least two years (no preliminary results available).
Authors' conclusions: In view of methodological deficiencies, and small sample size of the two included studies, we cannot draw any reliable conclusions regarding the optimal rate of tapering of AEDs. Using GRADE, we assessed the certainty of the evidence as very low for outcomes for which data were available. We judged both studies to be at an overall high risk of bias. Further studies are needed in adults and children to investigate the optimal rate of withdrawal of AEDs and to study the effects of variables such as seizure types, aetiology, intellectual disability, electroencephalography abnormalities, presence of neurological deficits, and other comorbidities on the rate of tapering.
Copyright © 2021 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
FAL: none known. EGT: none known. FB: none known.
Figures





Update of
-
Rapid versus slow withdrawal of antiepileptic drugs.Cochrane Database Syst Rev. 2020 Jan 23;1(1):CD005003. doi: 10.1002/14651858.CD005003.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Jan 10;1:CD005003. doi: 10.1002/14651858.CD005003.pub4. PMID: 31990368 Free PMC article. Updated.
References
References to studies included in this review
Serra 2005 {published data only}
Tennison 1994 {published data only}
References to studies excluded from this review
Aidaros 2010 {published data only}
-
- Aidaros MA, Siam AG. Effect of the duration of withdrawal of antiepileptic drugs on the risk of seizure recurrence in childhood epilepsy. Egyptian Journal of Neurology, Psychiatry and Neurosurgery 2010;47(4):593-8.
Braathen 1996 {published data only}
-
- Braathen G, Andersson T, Gylje H, Melander H, Naglo AS, Noren L, et al. Comparison between one and three years of treatment in uncomplicated childhood epilepsy: a prospective study. I. Outcome in different seizure types. Epilepsia 1996;37(9):822-32. [PMID: ] - PubMed
Gebremariam 1999 {published data only}
-
- Gebremariam A, Mengesha W, Enqusilassie F. Discontinuing anti-epileptic medication(s) in epileptic children: 18 versus 24 months. Annals of Tropical Paediatrics 1999;19(1):93-9. [PMID: ] - PubMed
Gherpelli 1992 {published data only}
-
- Gherpelli JL, Kok F, dal Forno S, Elkis LC, Lefevre BH, Diament AJ. Discontinuing medication in epileptic children: a study of risk factors related to recurrence. Epilepsia 1992;33(4):681-6. [PMID: ] - PubMed
He 2016 {published data only}
-
- He RQ, Zeng QY, Zhu P, Bao YX, Zheng RY, Xu HQ. Risk of seizure relapse after antiepileptic drug withdrawal in adult patients with focal epilepsy. Epilepsy & Behavior 2016;64(Pt A):233-8. [PMID: ] - PubMed
MRC 1991 {published data only}
-
- Medical Research Council Antiepileptic Drug Withdrawal Study Group. Randomised study of antiepileptic drug withdrawal in patients in remission. Lancet 1991;337(8751):1175-80. [PMID: ] - PubMed
Peters 1998 {published data only}
-
- Peters AC, Brouwer OF, Geerts AT, Arts WF, Stroink H, Donselaar CA. Randomized prospective study of early discontinuation of antiepileptic drugs in children with epilepsy. Neurology 1998;50(3):724-30. [PMID: ] - PubMed
Todt 1984 {published data only}
-
- Todt H. The late prognosis of epilepsy in childhood: results of a prospective follow-up study. Epilepsia 1984;25(2):137-44. [PMID: ] - PubMed
Verrotti 2000 {published data only}
-
- Verrotti A, Morresi S, Basciani F, Cutarella R, Morgese G, Chiarelli F. Discontinuation of anticonvulsant therapy in children with partial epilepsy. Neurology 2000;55(9):1393-5. [PMID: ] - PubMed
References to ongoing studies
Gasparini 2016 {published data only}
-
- Gasparini S, Ferlazzo E, Giussani G, Italiano D, Cianci V, Sueri C, et al. Rapid versus slow withdrawal of antiepileptic monotherapy in 2-year seizure-free adult patients with epilepsy (RASLOW) study: a pragmatic multicentre, prospective, randomized, controlled study. Neurological Sciences 2016;37(4):579-83. [DOI: 10.1007/s10072-016-2483-3] [PMID: ] - DOI - PubMed
Additional references
Arts 1988
-
- Arts WF, Visser LH, Loonen MC, Tjiam AT, Stroink H, Stuurman PM, et al. Follow-up of 146 children with epilepsy after withdrawal of antiepileptic therapy. Epilepsia 1988;29(3):244-50. [PMID: ] - PubMed
Beghi 2013
-
- Beghi E, Giussani G, Grosso S, Iudice A, La Neve A, Pisani F, Specchio LM, Verrotti A, Capovilla G, Michelucci R, Zaccara G. Withdrawal of antiepileptic drugs: guidelines of the Italian League Against Epilepsy. Epilepsia 2013;Suppl 7:2-12. - PubMed
Berg 1994
-
- Berg AT, Shinnar S. Relapse following discontinuation of antiepileptic drugs: a meta-analysis. Neurology 1994;44(4):601-8. [PMID: ] - PubMed
Bouma 1987
Brodie 2012
Callaghan 1988
-
- Callaghan N, Garrett A, Goggin T. Withdrawal of anticonvulsant drugs in patients free of seizures for two years: a prospective study. New England Journal of Medicine 1988;318(15):942-6. [PMID: ] - PubMed
Duncan 1987
-
- Duncan JS, Shorvon SD. Rates of antiepileptic drug reduction in active epilepsy – current practice. Epilepsy Research 1987;1(6):357-64. [PMID: ] - PubMed
Emerson 1981
-
- Emerson R, D'Souza BJ, Vining EP, Holden KR, Mellits ED, Freeman JM. Stopping medication in children with epilepsy: predictors of outcome. New England Journal of Medicine 1981;304(19):1125-9. [PMID: ] - PubMed
Fisher 2014
-
- Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 2014;55(4):475-82. [PMID: ] - PubMed
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Version accessed 16 July 2019. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Guyatt 2008
-
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al, GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924-6. [DOI: 10.1136/bmj.39489.470347.AD] [PMID: ] - DOI - PMC - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Juul‐Jensen 1964
-
- Juul-Jensen P. Frequency of recurrence after discontinuance of anti-convulsant therapy in patients with epileptic seizures. Epilepsia 1964;5:352-63. [PMID: ] - PubMed
Lefebvre 2021
-
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Technical supplement to chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston MS, Li T, Page MJ, et al. editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.
MRC 1993
NICE 2012
-
- NICE, The National Institute for Health and Care Excellence. NICE Clinical Guidelines, No. 137. London: National Institute for Health and Care Excellence (NICE), 2021.
Oller‐Daurella 1975
-
- Oller-Daurella L, Pamies R, Oller LF. Reduction or discontinuance of antiepileptic drugs in patients seizure-free for more than 5 years. In: Janz D, editors(s). Epileptology: Proceedings of the Seventh International Symposium on Epilepsy. Berlin: Georg Thieme Verlag, 1975:218-27.
Overweg 1981
-
- Overweg J, Rowan AJ, Binnie CD, Oosting J, Nagelkerke NJ. Prediction of seizure recurrence after withdrawal of antiepileptic drugs. In: Dam M, Gram L, Penry JK, editors(s). Advances in Epileptology: the XIIth Epilepsy International Symposium. New York: Raven Press, 1981:503-8.
Review Manager 2014 [Computer program]
-
- Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Shih 2009
-
- Shih JJ, Ochoa JG. A Systematic Review of Antiepileptic Drug Initiation and Withdrawal. Neurologist 2009;15(3):122-131. - PubMed
Shinnar 1994
-
- Shinnar S, Berg AT, Moshe SL, Kang H, O'Dell C, Alemany M, et al. Discontinuing antiepileptic drugs in children with epilepsy: a prospective study. Annals of Neurology 1994;35(5):534-45. [PMID: ] - PubMed
References to other published versions of this review
Ayuga Loro 2020
Ranganathan 2004
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical