

Association of a Third Dose of BNT162b2 Vaccine With Incidence of SARS-CoV-2 Infection Among Health Care Workers in Israel
- PMID: 35006256
- PMCID: PMC8749710
- DOI: 10.1001/jama.2021.23641
Association of a Third Dose of BNT162b2 Vaccine With Incidence of SARS-CoV-2 Infection Among Health Care Workers in Israel
Abstract
Importance: Administration of a BNT162b2 booster dose (Pfizer-BioNTech) to fully vaccinated individuals aged 60 years and older was significantly associated with lower risk of SARS-CoV-2 infection and severe illness. Data are lacking on the effectiveness of booster doses for younger individuals and health care workers.
Objective: To estimate the association of a BNT162b2 booster dose with SARS-CoV-2 infections among health care workers who were previously vaccinated with a 2-dose series of BNT162b2.
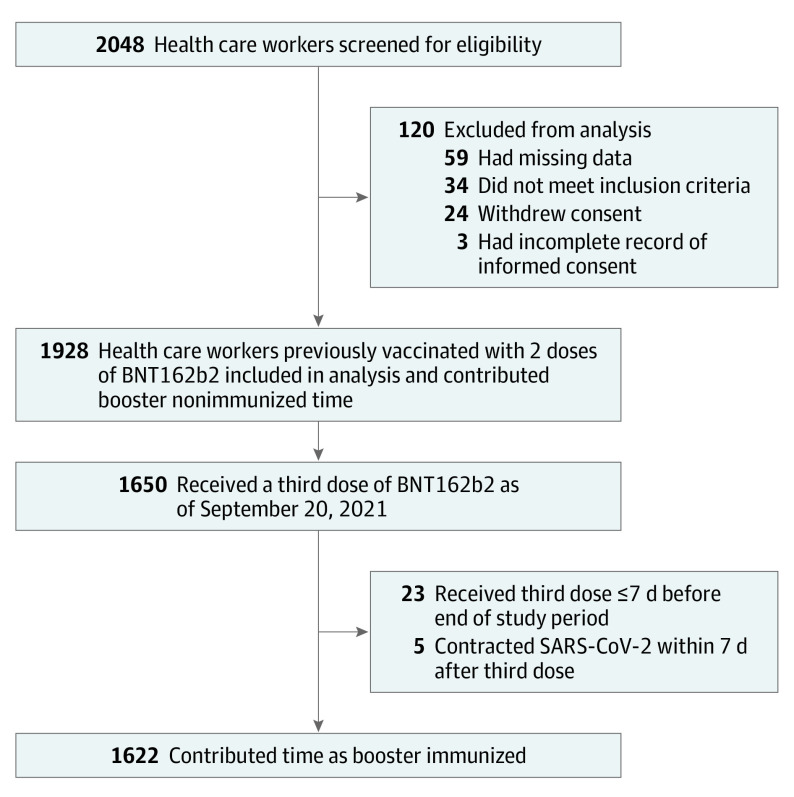
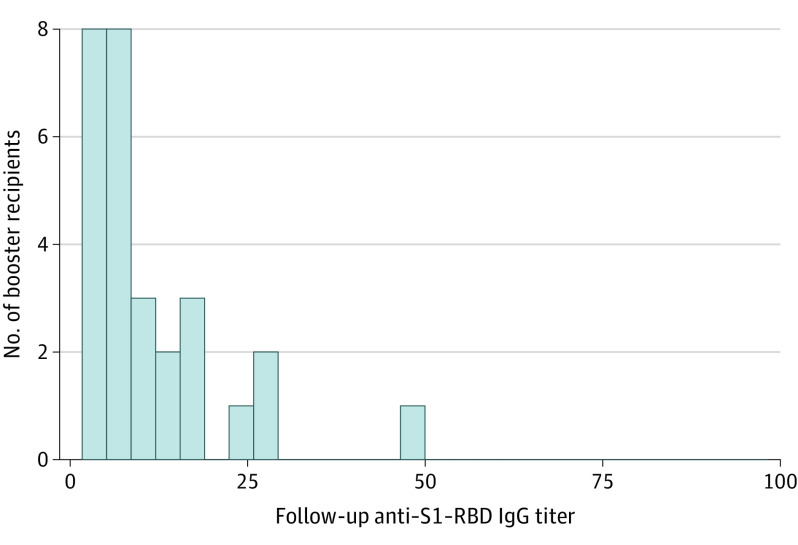
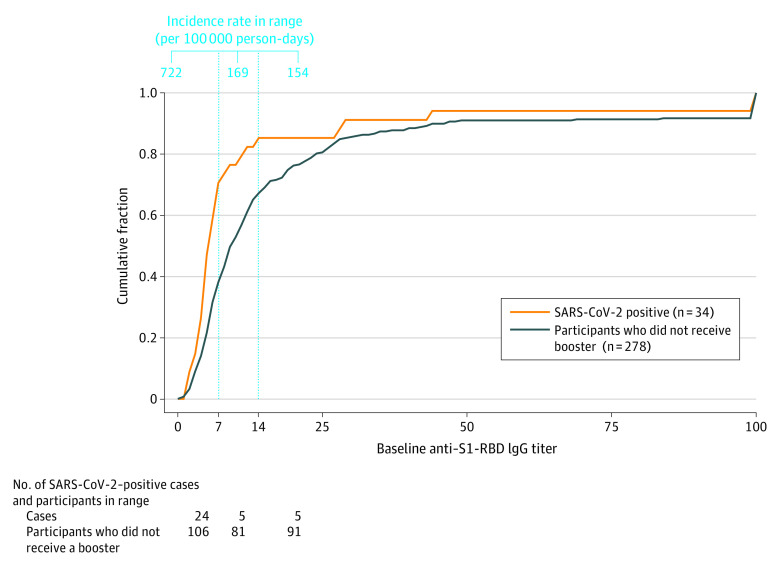
Design, setting, and participants: This was a prospective cohort study conducted at a tertiary medical center in Tel Aviv, Israel. The study cohort included 1928 immunocompetent health care workers who were previously vaccinated with a 2-dose series of BNT162b2, and had enrolled between August 8 and 19, 2021, with final follow-up reported through September 20, 2021. Screening for SARS-CoV-2 infection was performed every 14 days. Anti-spike protein receptor binding domain IgG titers were determined at baseline and 1 month after enrollment. Cox regression with time-dependent analysis was used to estimate hazard ratios of SARS-CoV-2 infection between booster-immunized status and 2-dose vaccinated (booster-nonimmunized) status.
Exposures: Vaccination with a booster dose of BNT162b2 vaccine.
Main outcomes and measures: The primary outcome was SARS-CoV-2 infection, as confirmed by reverse transcriptase-polymerase chain reaction.
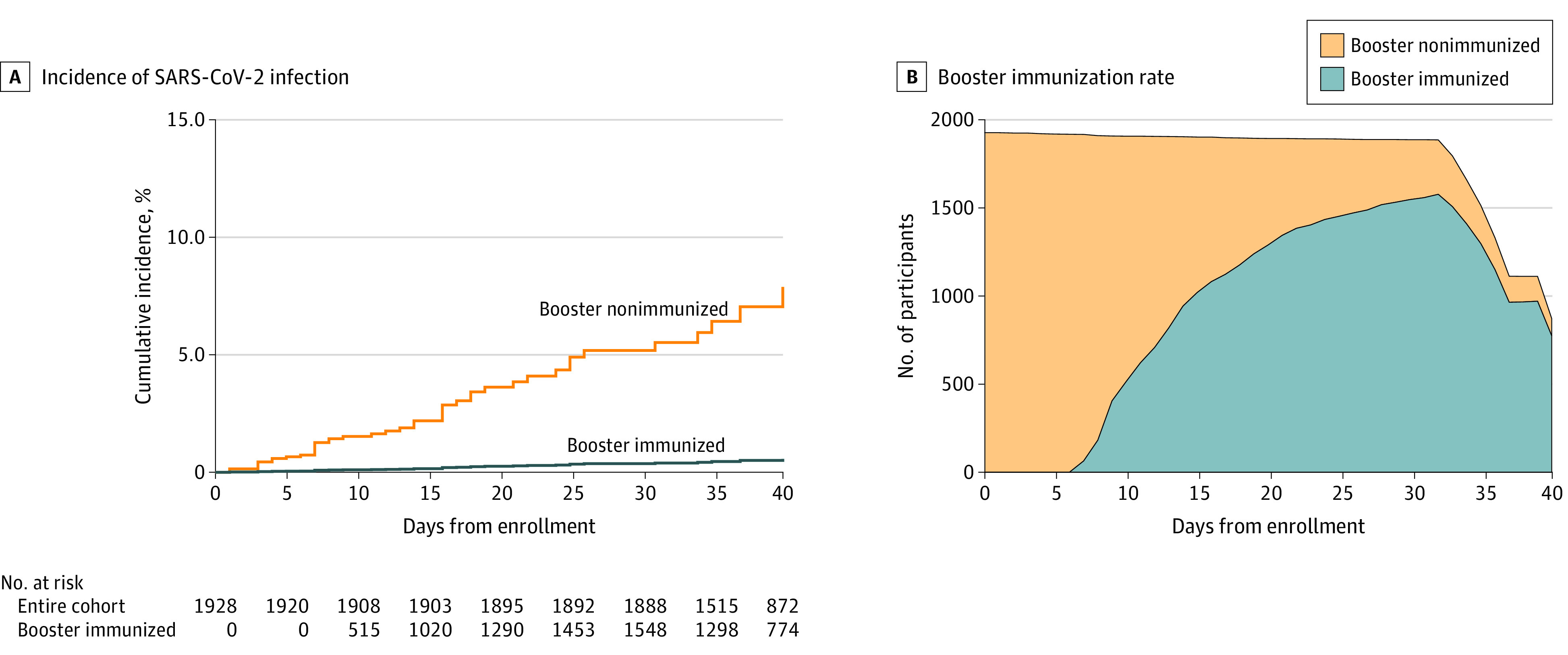
Results: Among 1928 participants, the median age was 44 years (IQR, 36-52 years) and 1381 were women (71.6%). Participants completed the 2-dose vaccination series a median of 210 days (IQR, 205-213 days) before study enrollment. A total of 1650 participants (85.6%) received the booster dose. During a median follow-up of 39 days (IQR, 35-41 days), SARS-CoV-2 infection occurred in 44 participants (incidence rate, 60.2 per 100 000 person-days); 31 (70.5%) were symptomatic. Five SARS-CoV-2 infections occurred in booster-immunized participants and 39 in booster-nonimmunized participants (incidence rate, 12.8 vs 116 per 100 000 person-days, respectively). In a time-dependent Cox regression analysis, the adjusted hazard ratio of SARS-CoV-2 infection for booster-immunized vs booster-nonimmunized participants was 0.07 (95% CI, 0.02-0.20).
Conclusions and relevance: Among health care workers at a single center in Israel who were previously vaccinated with a 2-dose series of BNT162b2, administration of a booster dose compared with not receiving one was associated with a significantly lower rate of SARS-CoV-2 infection over a median of 39 days of follow-up. Ongoing surveillance is required to assess durability of the findings.
Conflict of interest statement
Figures
Comment in
-
Booster Vaccination to Reduce SARS-CoV-2 Transmission and Infection.JAMA. 2022 Jan 25;327(4):327-328. doi: 10.1001/jama.2021.23726. JAMA. 2022. PMID: 35006269 No abstract available.
References
-
- Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397(10287):1819-1829. doi: 10.1016/S0140-6736(21)00947-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
