

Effect of a Ward-Based Program on Hospital-Associated Complications and Length of Stay for Older Inpatients: The Cluster Randomized CHERISH Trial
- PMID: 35006265
- PMCID: PMC8749692
- DOI: 10.1001/jamainternmed.2021.7556
Effect of a Ward-Based Program on Hospital-Associated Complications and Length of Stay for Older Inpatients: The Cluster Randomized CHERISH Trial
Abstract
Importance: Hospital-associated complications of older people (HAC-OPs) include delirium, hospital-associated disability, incontinence, pressure injuries, and falls. These complications may be preventable by age-friendly principles of care, including early mobility, good nutrition and hydration, and meaningful cognitive engagement; however, implementation is challenging.
Objectives: To implement and evaluate a ward-based improvement program ("Eat Walk Engage") to more consistently deliver age-friendly principles of care to older individuals in acute inpatient wards.
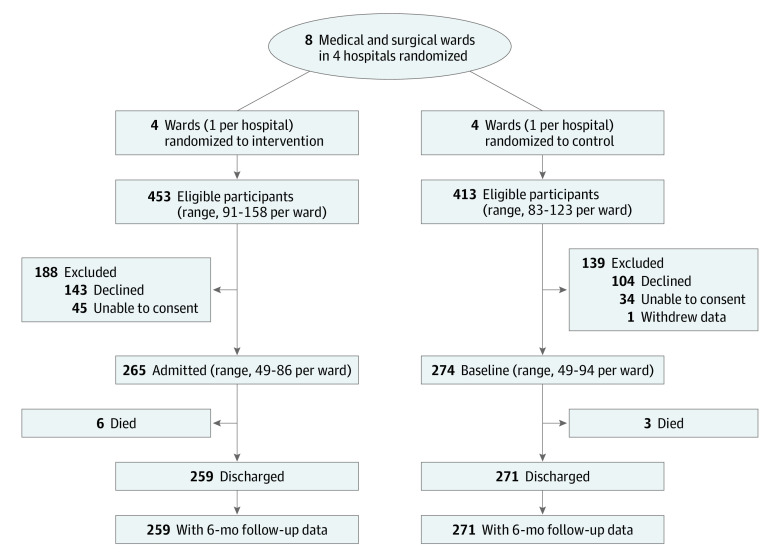
Design, setting, and participants: This cluster randomized CHERISH (Collaboration for Hospitalised Elders Reducing the Impact of Stays in Hospital) trial enrolled 539 consecutive inpatients aged 65 years or older, admitted for 3 days or more to study wards, from October 2, 2016, to April 3, 2017, with a 6-month follow-up. The study wards comprised 8 acute medical and surgical wards in 4 Australian public hospitals. Randomization was stratified by hospital, providing 4 clusters in intervention and in control groups. Statistical analysis was performed from August 28, 2018, to October 17, 2021, on an intention-to-treat basis.
Intervention: A trained facilitator supported a multidisciplinary work group on each intervention ward to improve the care practices, environment, and culture to support key age-friendly principles.
Main outcomes and measures: Primary outcomes were incidence of any HAC-OP and length of stay. Secondary outcomes were incidence of individual HAC-OPs, facility discharge, 6-month mortality, and all-cause readmission. Outcomes were analyzed at the individual level, adjusted for confounders and clustering.
Results: A total of 265 participants on 4 intervention wards (124 women [46.8%]; mean [SD] age, 75.9 [7.3] years) and 274 participants on 4 control wards (145 women [52.9%]; mean [SD] age, 78.0 [8.2] years) were enrolled. The composite primary outcome of any HAC-OP occurred for 115 of 248 intervention participants (46.4%) and 129 of 249 control participants (51.8%) (intervention group: adjusted odds ratio, 1.07; 95% CI, 0.71-1.61). The median length of stay was 6 days (IQR, 4-9 days) for the intervention group and 7 days (IQR, 5-10 days) for the control group (adjusted hazard ratio, 0.96; 95% credible interval, 0.80-1.15). The incidence of delirium was significantly lower for intervention participants (adjusted odds ratio, 0.53; 95% CI, 0.31-0.90). There were no significant differences in other individual HAC-OPs, facility discharge, mortality, or readmissions.
Conclusions and relevance: The Eat Walk Engage program did not reduce the composite primary outcome of any HAC-OP or length of stay, but there was a significant reduction in the incidence of delirium.
Trial registration: anzctr.org.au Identifier: ACTRN12615000879561.
Conflict of interest statement
Figures
References
-
- Parke B, Chappell NL. Transactions between older people and the hospital environment: a social ecological analysis. J Aging Stud. 2010;24(2):115-124. doi: 10.1016/j.jaging.2008.09.003 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
