

The bone marrow niche components are adversely affected in sepsis
- PMID: 35006437
- PMCID: PMC8607421
- DOI: 10.1186/s43556-020-00010-3
The bone marrow niche components are adversely affected in sepsis
Erratum in
-
Author Correction: The bone marrow niche components are adversely affected in sepsis.Mol Biomed. 2025 Nov 4;6(1):96. doi: 10.1186/s43556-025-00304-4. Mol Biomed. 2025. PMID: 41186807 Free PMC article. No abstract available.
Abstract
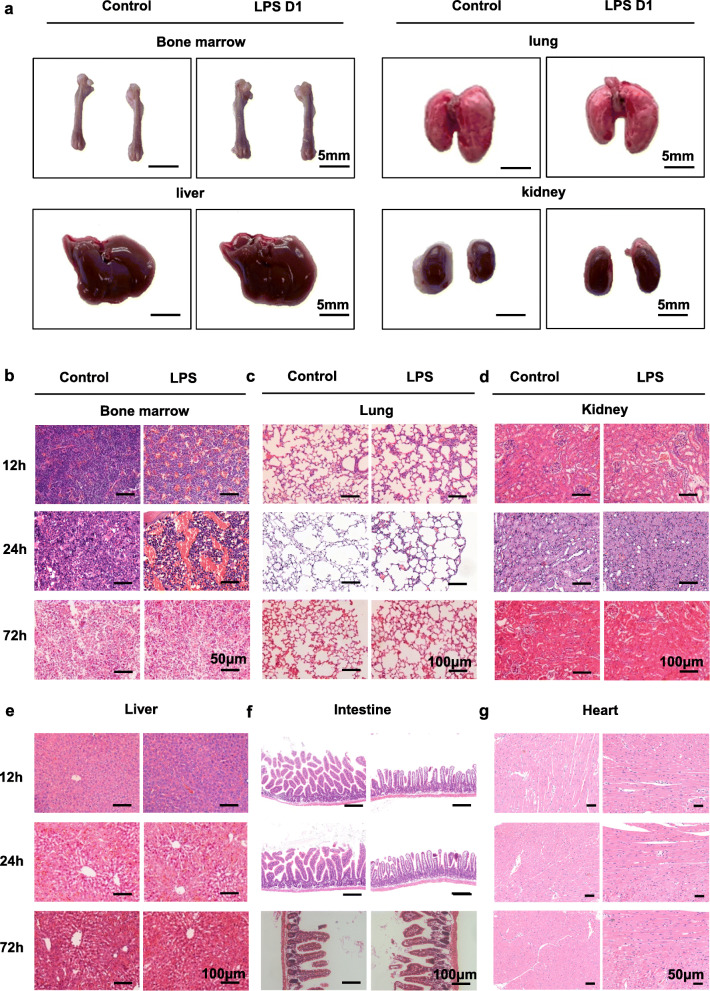
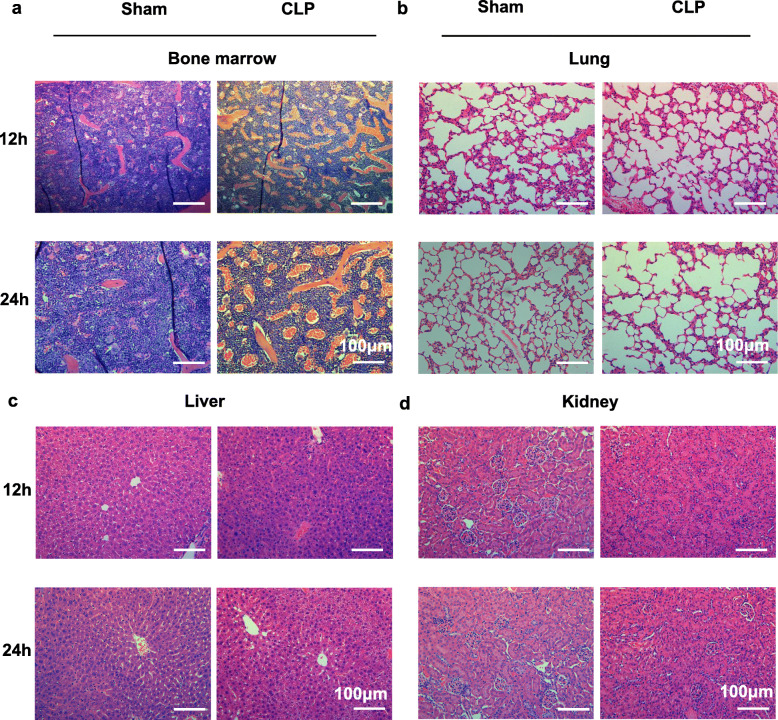
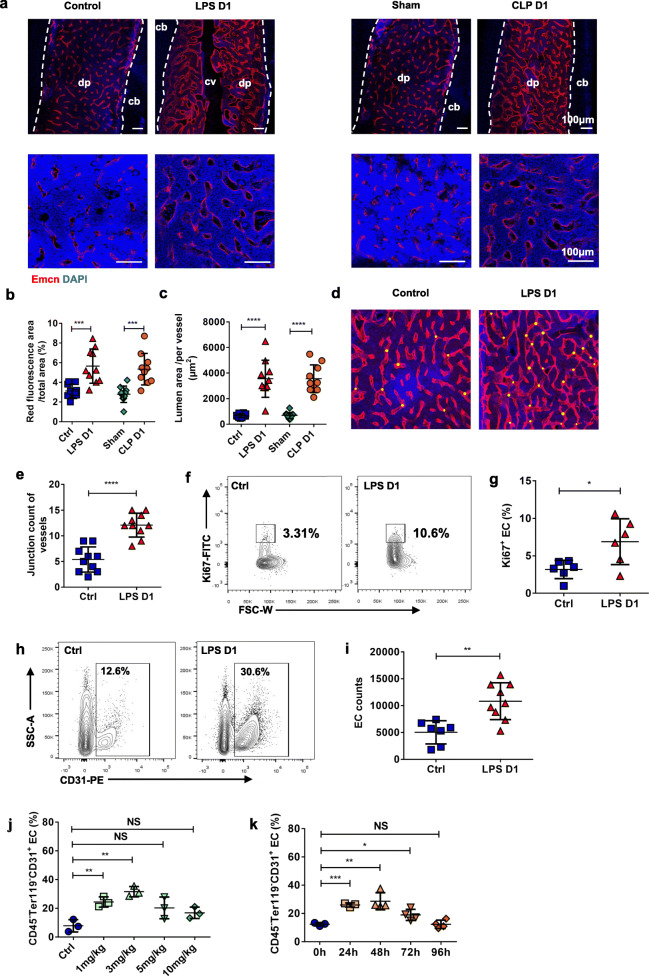
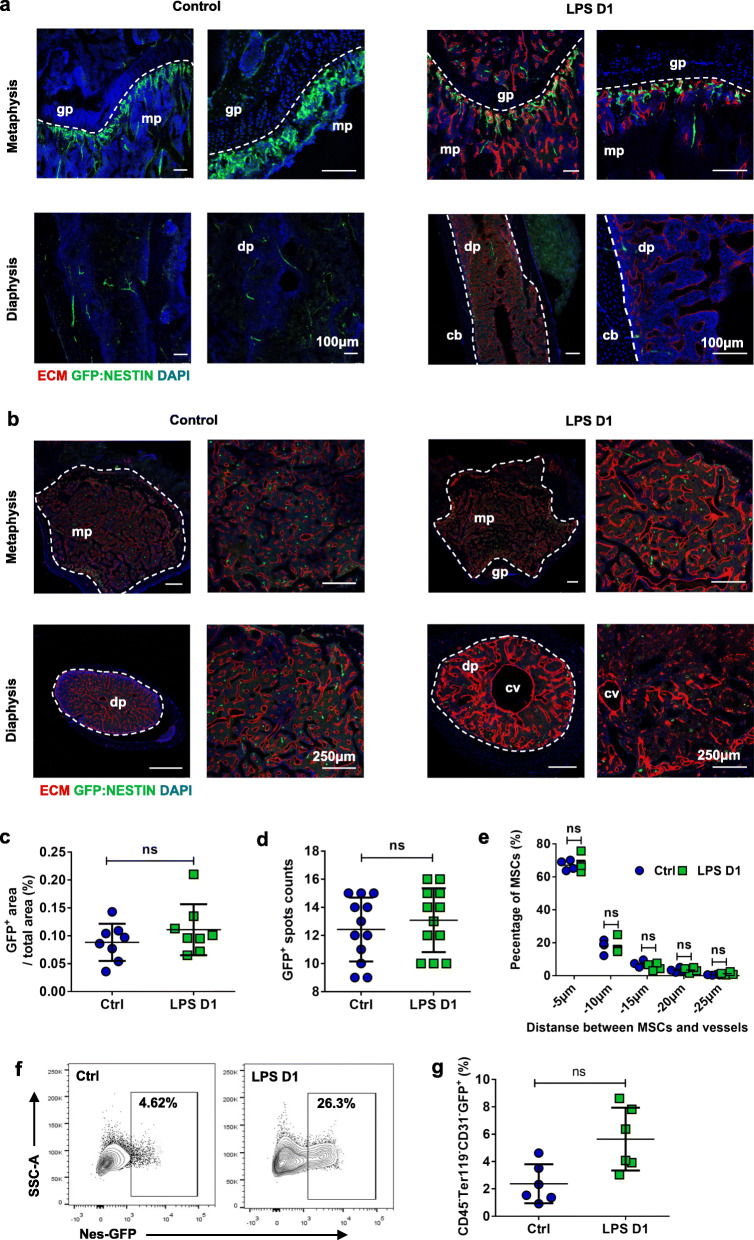
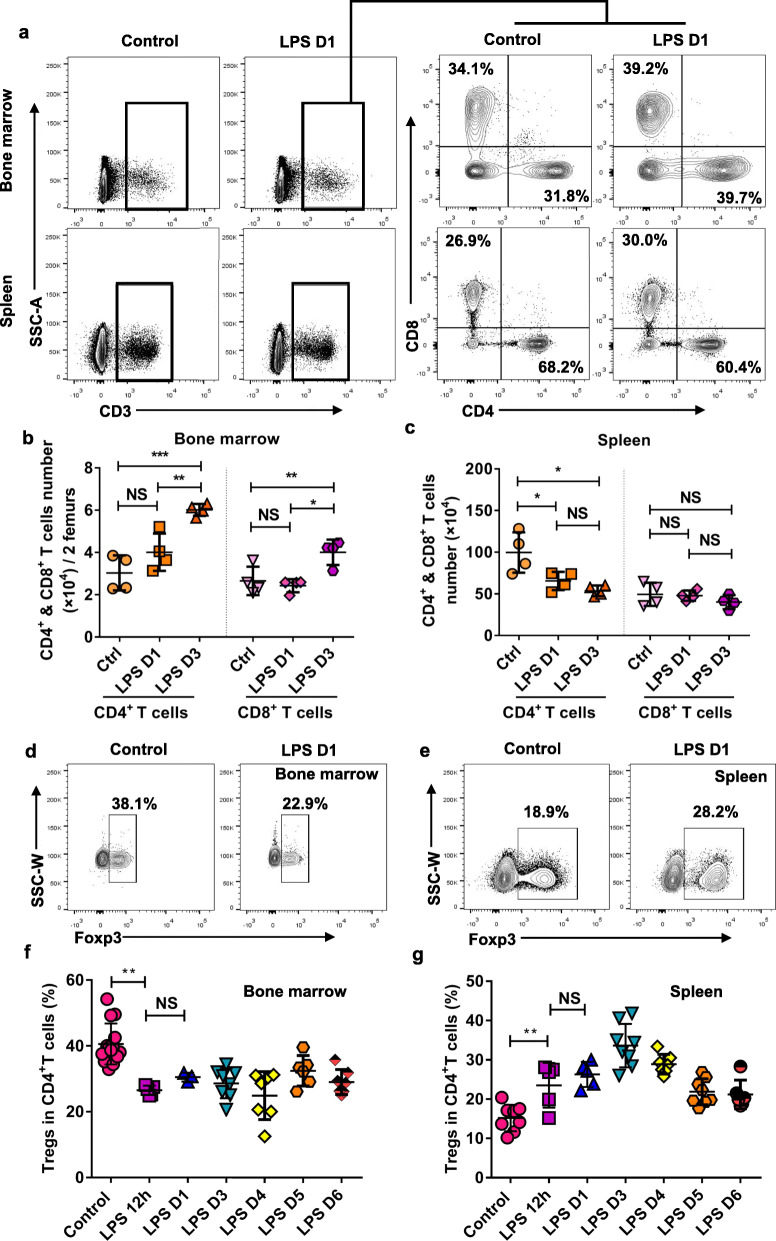
Multiple organ dysfunction is an important cause of death in patients with sepsis. Currently, few studies have focused on the impact of sepsis on bone marrow (BM), especially on the cell components of BM niche. In this study, we performed mouse sepsis models by intraperitoneal injection of LPS and cecal ligation and puncture (CLP). The changes of niche major components in the mouse BM among vascular structures, mesenchymal stem cells and Treg cells were observed and analyzed. The results showed that pathological changes in BM was earlier and more prominent than in other organs, and various cell components of the BM niche changed significantly, of which vascular endothelial cells increased transiently with vascular remodeling and the regulatory T cells decreased over a long period of time. These results indicated that the components of the BM niche underwent series of adaptive changes in sepsis.
Keywords: Bone marrow niche; Lipopolysaccharide (LPS); Mouse model; Sepsis.
© 2020. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous