

Triiodothyronine (T3), inflammation and mortality risk in patients with acute myocardial infarction
- PMID: 35007210
- PMCID: PMC9142797
- DOI: 10.1530/ETJ-21-0085
Triiodothyronine (T3), inflammation and mortality risk in patients with acute myocardial infarction
Abstract
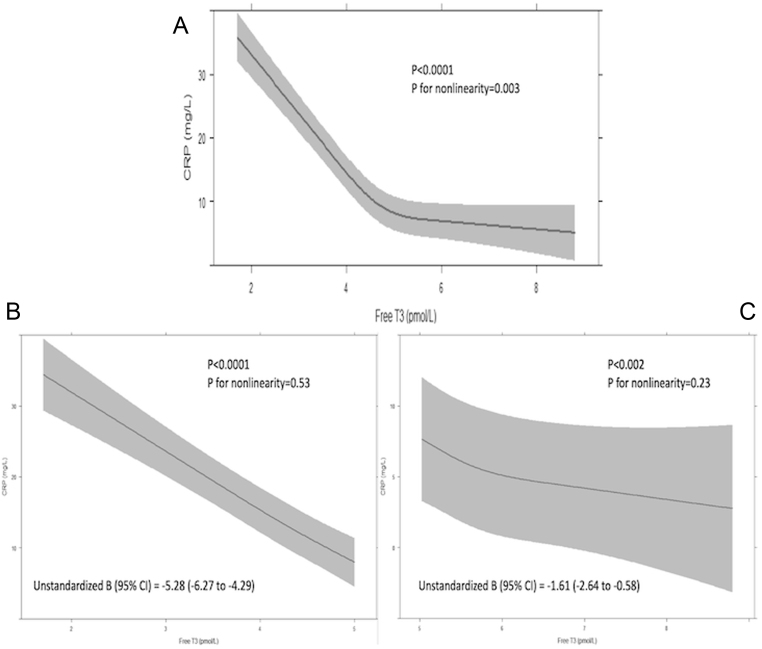
Objectives: To study the relationship between serum-free T3 (FT3), C-reactive protein (CRP) and all-cause mortality in patients with acute myocardial infarction (AMI).
Design: Prospective multicentre longitudinal cohort study.
Methods: Between December 2014 and December 2016, thyroid function and CRP were analysed in AMI (both ST-elevation (STEMI) and non-ST-elevation) patients from the Thyroxine in Acute Myocardial Infarction study. The relationship of FT3 and CRP at baseline with all-cause mortality up to June 2020 was assessed. Mediation analysis was performed to evaluate if CRP mediated the relationship between FT3 and mortality.
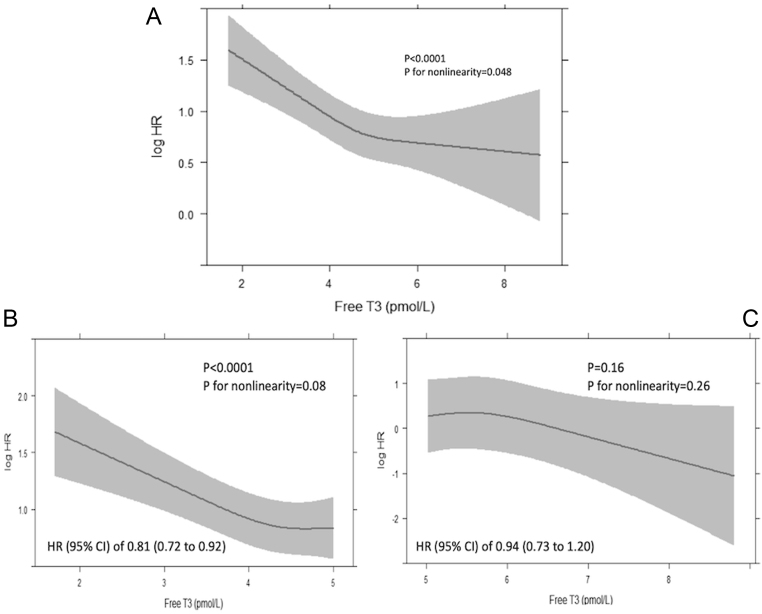
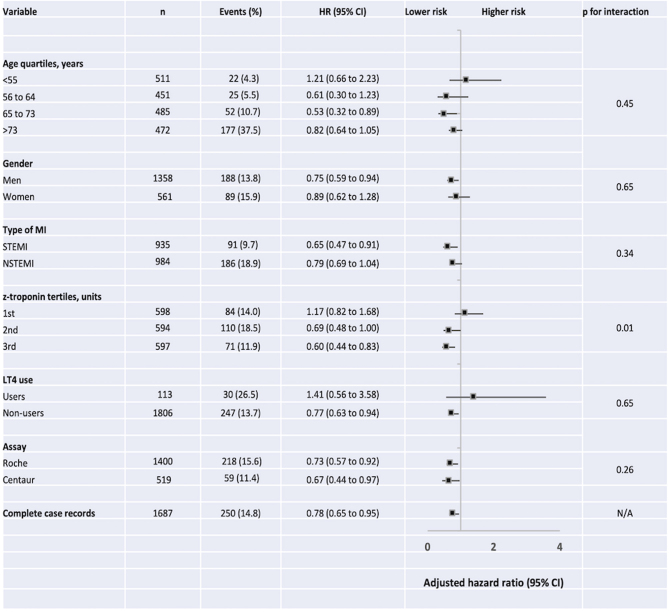
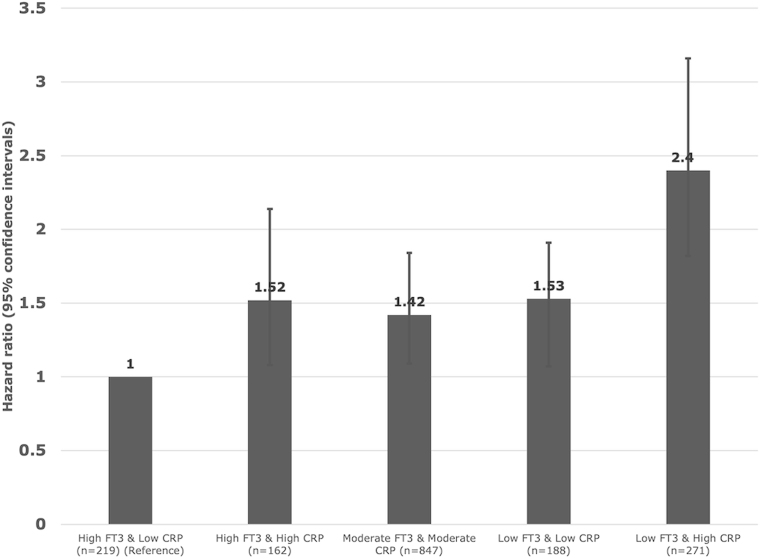
Results: In 1919 AMI patients (29.2% women, mean (s.d.) age: 64.2 (12.1) years and 48.7% STEMI) followed over a median (interquartile range) period of 51 (46-58) months, there were 277 (14.4%) deaths. Overall, lower serum FT3 and higher CRP levels were associated with higher risk of mortality. When divided the patients into tertiles based on the levels of FT3 and CRP; the group with the lowest FT3 and highest CRP levels had a 2.5-fold increase in mortality risk (adjusted hazard ratio (95% CI) of 2.48 (1.82-3.16)) compared to the group with the highest FT3 and lowest CRP values. CRP mediated 9.8% (95% CI: 6.1-15.0%) of the relationship between FT3 and mortality.
Conclusions: In AMI patients, lower serum FT3 levels on admission are associated with a higher mortality risk, which is partly mediated by inflammation. Adequately designed trials to explore the potential benefits of T3 in AMI patients are required.
Keywords: acute myocardial infarction; inflammation; mortality; triiodothyronine.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
