

Correlation between fetal heart rate evolution patterns and magnetic resonance imaging findings in severe cerebral palsy: A longitudinal study
- PMID: 35007405
- PMCID: PMC9545186
- DOI: 10.1111/1471-0528.17089
Correlation between fetal heart rate evolution patterns and magnetic resonance imaging findings in severe cerebral palsy: A longitudinal study
Abstract
Objective: To investigate the association between hypoxic-ischaemic insult timing and brain injury type in infants with severe cerebral palsy (CP).
Design: Longitudinal study.
Setting: Database of the Recurrence Prevention Committee, Japan Obstetric Compensation System for Cerebral Palsy.
Sample: Infants with severe CP born at ≥34 weeks of gestation.
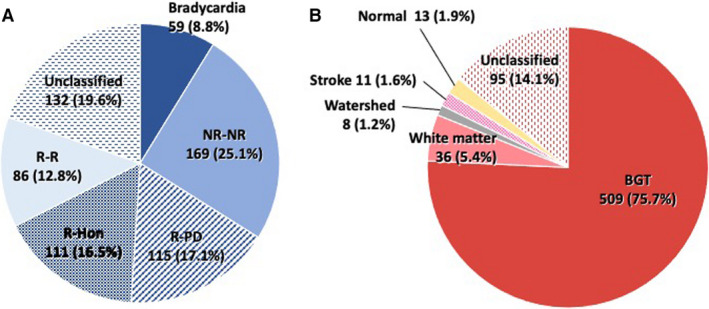
Methods: The intrapartum fetal heart rate (FHR) strips were categorised as continuous bradycardia; persistently non-reassuring (NR-NR); reassuring-prolonged deceleration (R-PD); Hon's pattern (R-Hon); persistently reassuring (R-R); and unclassified. The brain magnetic resonance imaging (MRI) scans were categorised based on the predominant site involved: basal ganglia-thalamus (BGT); white matter (WM); watershed (WS); stroke; normal; and unclassified.
Main outcome measures: Manifestations of the brain MRI types and the association between FHR evolution pattern and MRI type were analysed.
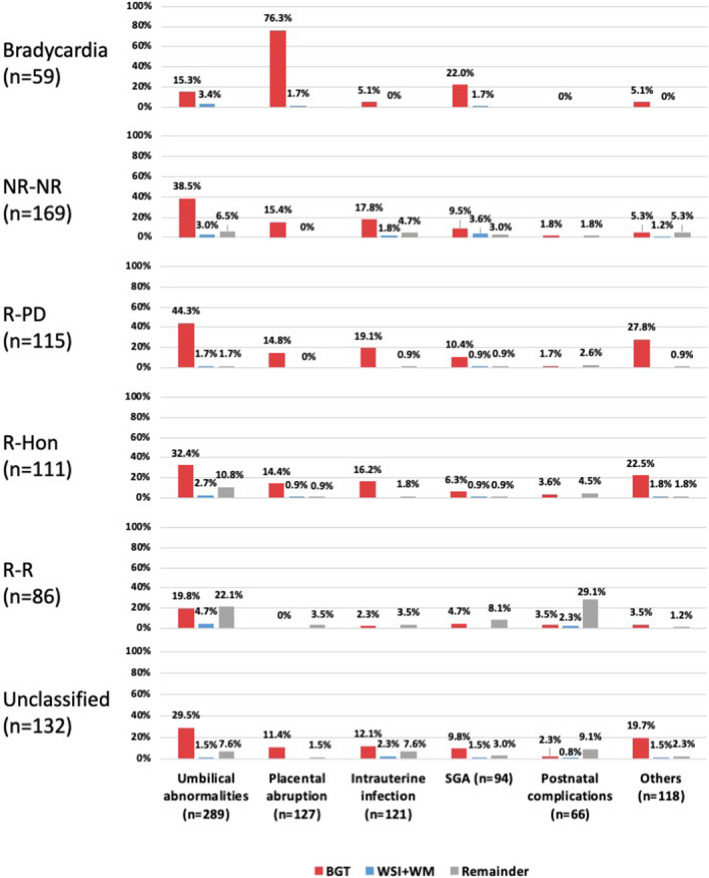
Results: Among 672 eligible infants, 76% had BGT-dominant injury, 5.4% WM, 1.2% WS, 1.6% stroke, 1.9% normal, and 14% unclassified. Placental abruption and small-for-gestational age were associated with an increased (adjusted odds ratio [aOR] 8.02) and decreased (aOR 0.38) risk of BGT injury, respectively. The majority of infants had BGT injury in most FHR groups (bradycardia, 97%; NR-NR, 75%; R-PD, 90%; R-Hon, 76%; and R-R, 45%). The risk profiles in case of BGT in the NR-NR group were similar to those in the R-PD and R-Hon groups.
Conclusion: BGT-dominant brain damage accounted for three-fourths of the cases of CP in term or near-term infants, even in prenatal onset cases. Hypoxic-ischaemic insult has a major impact on CP development during the antenatal period.
Tweetable abstract: Basal ganglia-thalamus injury constitutes 76% of severe cerebral palsy cases, predominant even in antenatal-onset cases.
Keywords: basal ganglia; brain injuries; cardiotocograph; cerebral palsy; hypoxia-ischaemia; infant; perinatal; thalamus.
© 2022 The Authors. BJOG: An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd.
Conflict of interest statement
None declared. Completed disclosure of interest forms are available to view online as supporting information.
Figures
Similar articles
-
Fetal heart rate evolution and brain imaging findings in preterm infants with severe cerebral palsy.Am J Obstet Gynecol. 2023 May;228(5):583.e1-583.e14. doi: 10.1016/j.ajog.2022.11.1277. Epub 2022 Nov 9. Am J Obstet Gynecol. 2023. PMID: 36370872
-
Fetal heart rate pattern in term or near-term cerebral palsy: a nationwide cohort study.Am J Obstet Gynecol. 2020 Dec;223(6):907.e1-907.e13. doi: 10.1016/j.ajog.2020.05.059. Epub 2020 Jun 1. Am J Obstet Gynecol. 2020. PMID: 32497609
-
Placental pathology in full-term infants with hypoxic-ischemic neonatal encephalopathy and association with magnetic resonance imaging pattern of brain injury.J Pediatr. 2013 Oct;163(4):968-95.e2. doi: 10.1016/j.jpeds.2013.06.010. Epub 2013 Jul 25. J Pediatr. 2013. PMID: 23891350
-
Defining cerebral palsy: pathogenesis, pathophysiology and new intervention.Minerva Ginecol. 2009 Oct;61(5):421-9. Minerva Ginecol. 2009. PMID: 19749673 Review.
-
Optimizing the management of acute, prolonged decelerations and fetal bradycardia based on the understanding of fetal pathophysiology.Am J Obstet Gynecol. 2023 Jun;228(6):645-656. doi: 10.1016/j.ajog.2022.05.014. Am J Obstet Gynecol. 2023. PMID: 37270260 Review.
Cited by
-
Types of intrapartum hypoxia in the newborn at term with metabolic acidemia: A retrospective study.Acta Obstet Gynecol Scand. 2022 Nov;101(11):1276-1281. doi: 10.1111/aogs.14436. Epub 2022 Aug 25. Acta Obstet Gynecol Scand. 2022. PMID: 36004701 Free PMC article.
-
Circadian patterns of heart rate variability in fetal sheep after hypoxia-ischaemia: A biomarker of evolving brain injury.J Physiol. 2024 Dec;602(23):6553-6569. doi: 10.1113/JP284560. Epub 2023 Jul 11. J Physiol. 2024. PMID: 37432936 Free PMC article.
References
-
- Kodama Y, Sameshima H, Ikeda T, Ikenoue T. Intrapartum fetal heart rate patterns in infants (> or =34 weeks) with poor neurological outcome. Early Hum Dev. 2009;85(4):235–8. - PubMed
-
- McIntyre S, Blair E, Badawi N, Keogh J, Nelson KB. Antecedents of cerebral palsy and perinatal death in term and late preterm singletons. Obstet Gynecol. 2013;122(4):869–77. - PubMed
-
- MacLennan AH, Thompson SC, Gecz J. Cerebral palsy: causes, pathways, and the role of genetic variants. Am J Obstet Gynecol. 2015;213(6):779–88. - PubMed
-
- Korzeniewski SJ, Slaughter J, Lenski M, Haak P, Paneth N. The complex aetiology of cerebral palsy. Nat Rev Neurol. 2018;14(9):528–43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
