

Prenatal phthalate exposure in relation to placental corticotropin releasing hormone (pCRH) in the CANDLE cohort
- PMID: 35007898
- PMCID: PMC8821329
- DOI: 10.1016/j.envint.2022.107078
Prenatal phthalate exposure in relation to placental corticotropin releasing hormone (pCRH) in the CANDLE cohort
Abstract
Context: Phthalates may disrupt maternal-fetal-placental endocrine pathways, affecting pregnancy outcomes and child development. Placental corticotropin releasing hormone (pCRH) is critical for healthy pregnancy and child development, but understudied as a target of endocrine disruption.
Objective: To examine phthalate metabolite concentrations (as mixtures and individually) in relation to pCRH.
Design: Secondary data analysis from a prospective cohort study.
Setting: Prenatal clinics in Tennessee, USA.
Patients: 1018 pregnant women (61.4% non-Hispanic Black, 32% non-Hispanic White, 6.6% other) participated in the CANDLE study and provided data. Inclusion criteria included: low-medical-risk singleton pregnancy, age 16-40, and gestational weeks 16-29.
Intervention: None.
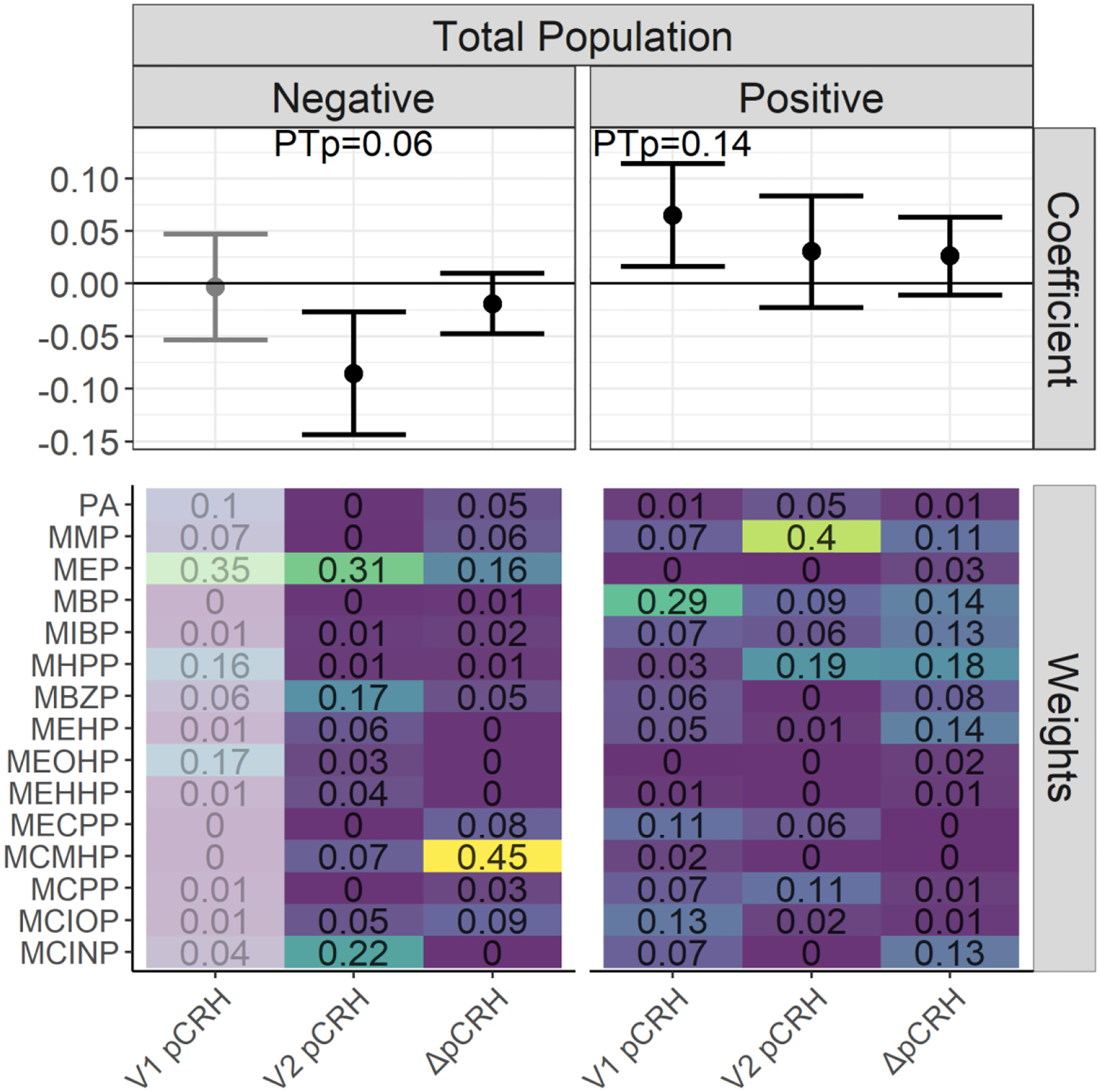
Main outcome measures: Plasma pCRH at two visits (mean gestational ages 23.0 and 31.8 weeks) and change in pCRH between visits (ΔpCRH).
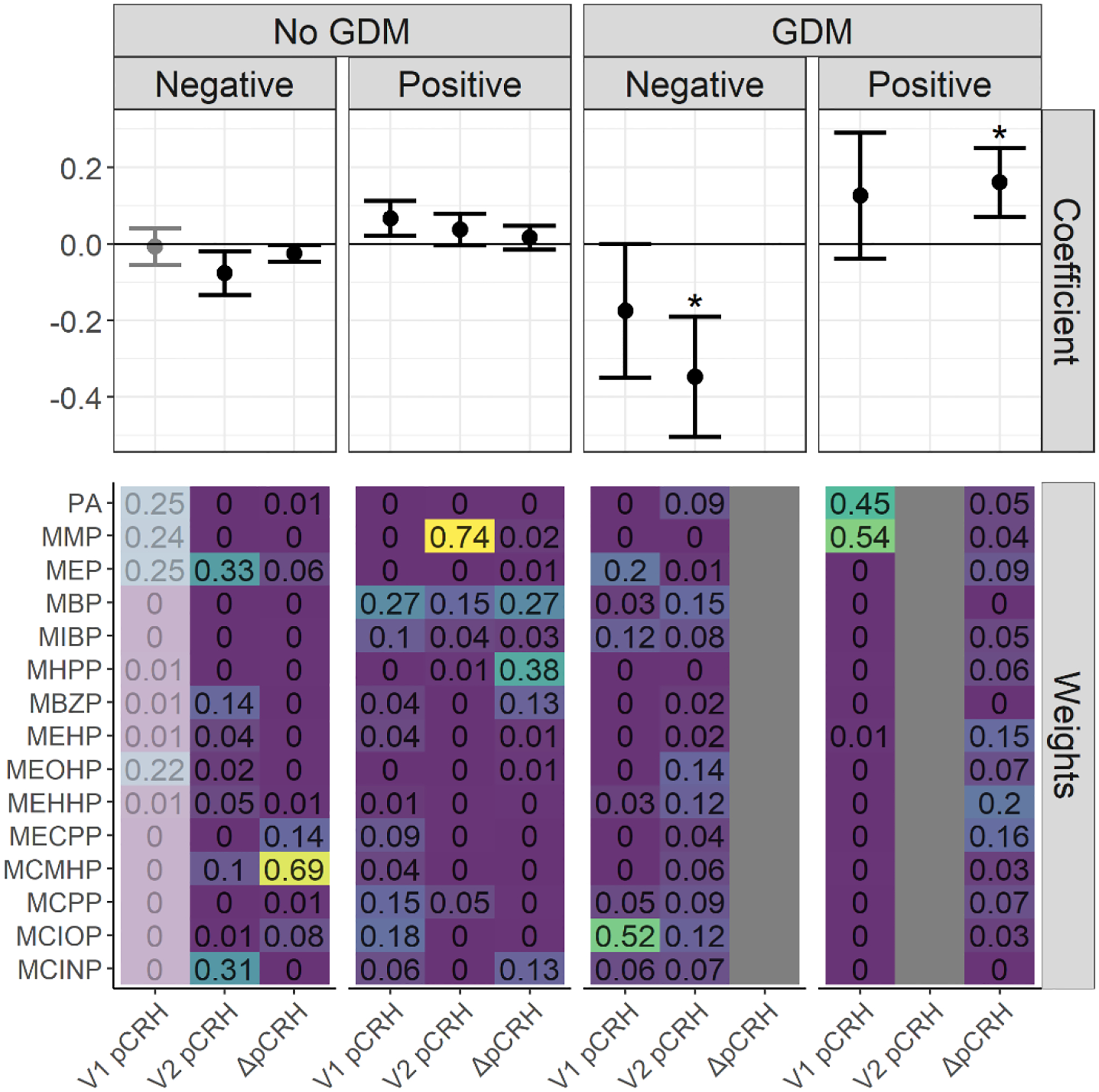
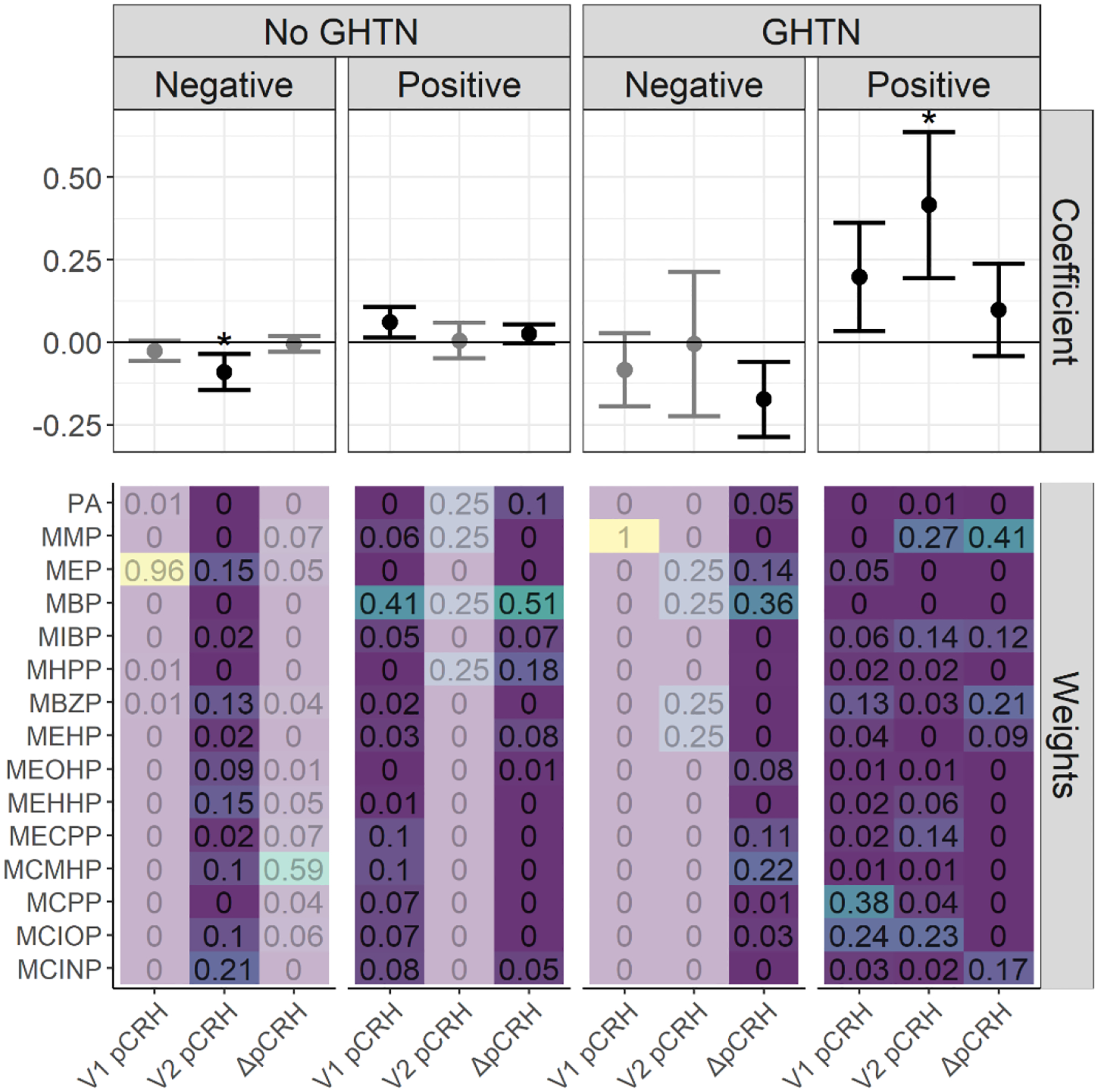
Results: In weighted quantile sums (WQS) regression models, phthalate mixtures were associated with higher pCRH at Visit 1 (β = 0.07, 95 %CI: 0.02, 0.11) but lower pCRH at Visit 2 (β = -0.08, 95 %CI: -0.14, -0.02). In stratified analyses, among women with gestational diabetes (n = 59), phthalate mixtures were associated with lower pCRH at Visit 1 (β = -0.17, 95 %CI: -0.35, 0.0006) and Visit 2 (β = -0.35, 95 %CI: -0.50, -0.19), as well as greater ΔpCRH (β = 0.16, 95 %CI: 0.07, 0.25). Among women with gestational hypertension (n = 102), phthalate mixtures were associated with higher pCRH at Visit 1 (β = 0.20, 95 %CI: 0.03, 0.36) and Visit 2 (β = 0.42; 95 %CI: 0.19, 0.64) and lower ΔpCRH (β = -0.17, 95 %CI: -0.29, -0.06). Significant interactions between individual phthalate metabolites and pregnancy complications were observed.
Conclusions: Phthalates may impact placental CRH secretion, with differing effects across pregnancy. Differences in results between women with and without gestational diabetes and gestational hypertension suggest a need for further research examining whether women with pregnancy complications may be more vulnerable to endocrine-disrupting effects of phthalates.
Keywords: Corticotropin releasing hormone; Endocrine disrupting chemicals; Phthalates; Placenta; Pregnancy complications.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Figures
References
-
- Arbuckle TE, Davis K, Marro L, Fisher M, Legrand M, LeBlanc A, Gaudreau E, Foster WG, Choeurng V, Fraser WD. Phthalate and bisphenol A exposure among pregnant women in Canada--results from the MIREC study. Environ Int. 2014;68:55–65. - PubMed
