

Prognostication in Acute Neurological Emergencies
- PMID: 35007934
- PMCID: PMC8837701
- DOI: 10.1016/j.jstrokecerebrovasdis.2021.106277
Prognostication in Acute Neurological Emergencies
Abstract
Background: For patients with acute, serious neurological conditions presenting to the emergency department (ED), prognostication is typically based on clinical experience, scoring systems and patient co-morbidities. Because estimating a poor prognosis influences caregiver decisions to withdraw life-sustaining therapy, we investigated the consistency of prognostication across a spectrum of neurology physicians.
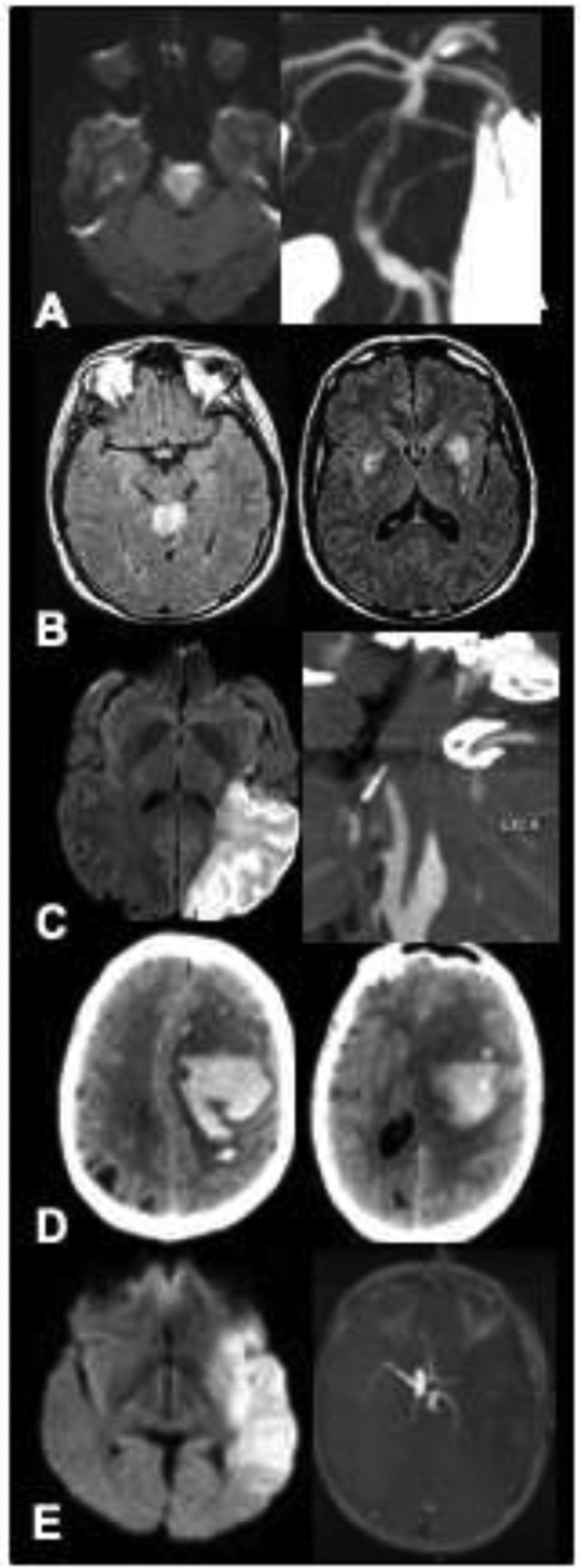
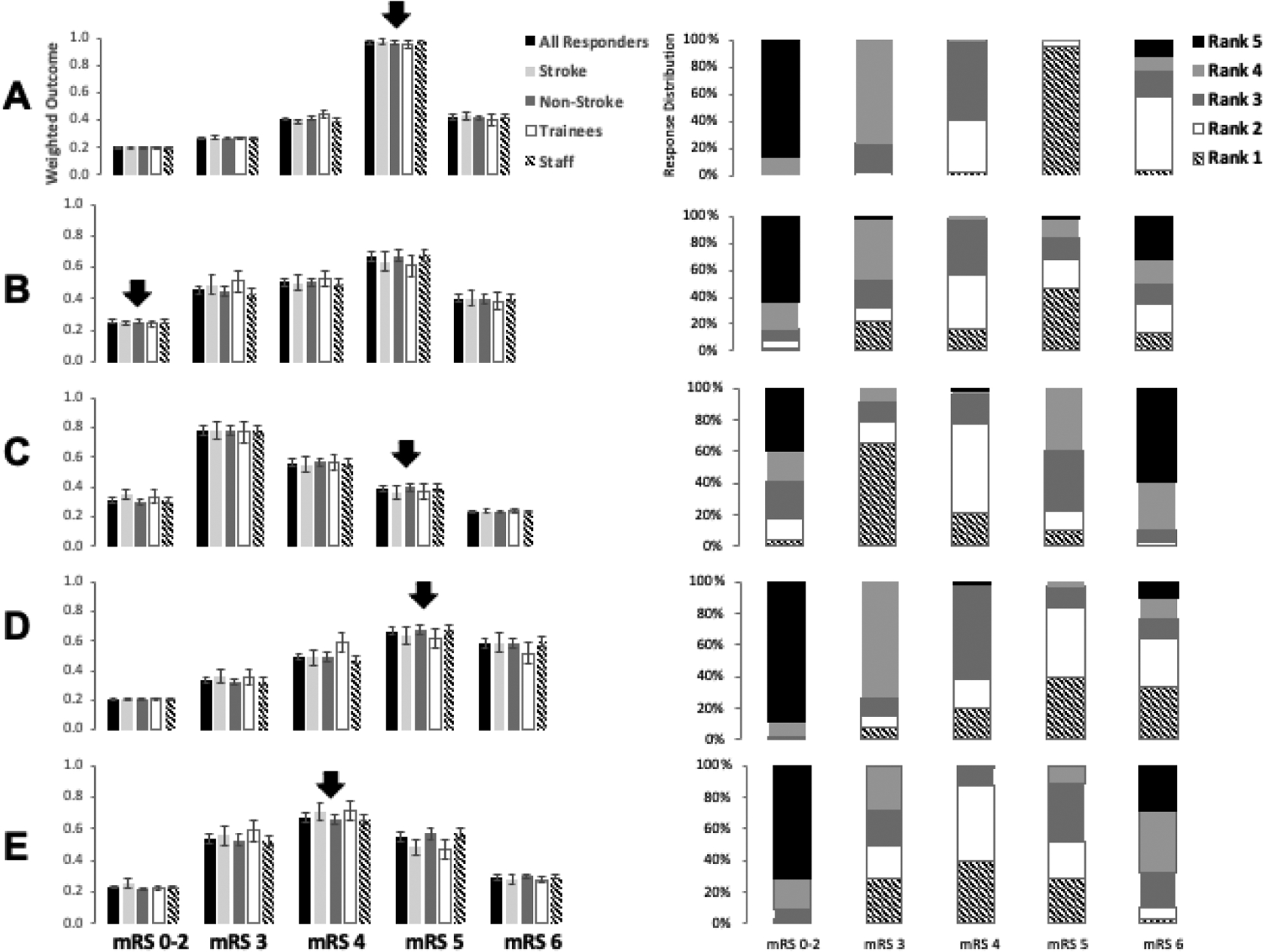
Methods: Five acute neurological presentations (2 with large hemispheric infarction; 1 with brainstem infarction, 1 with lobar hemorrhage, and 1 with hypoxic-ischemic encephalopathy) were selected for a department-wide prognostication simulation exercise. All had presented to our tertiary care hospital's ED, where a poor outcome was predicted by the ED neurology team within 24 hours of onset. Relevant clinical, laboratory and imaging data available before ED prognostication were presented on a web-based platform to 120 providers blinded to the actual outcome. The provider was requested to rank-order, from most to least likely, the predicted 90-day modified Rankin Scale (mRS) score. To determine the accuracy of individual outcome predictions we compared the patient's the actual 90-day mRS score to highest ranked predicted mRS score. Additionally, the group's "weighted" outcomes, accounting for the entire spectrum of mRS scores ranked by all respondents, were compared to the actual outcome for each case. Consistency was compared between pre-specified provider roles: neurology trainees versus faculty; non-vascular versus vascular faculty.
Results: Responses ranged from 106-110 per case. Individual predictions were highly variable, with predictions matching the actual mRS scores in as low as 2% of respondents in one case and 95% in another case. However, as a group, the weighted outcome matched the actual mRS score in 3 of 5 cases (60%). There was no significant difference between subgroups based on expertise (stroke/neurocritical care versus other) or experience (faculty versus trainee) in 4 of 5 cases.
Conclusion: Acute neuro-prognostication is highly variable and often inaccurate among neurology providers. Significant differences are not attributable to experience or subspecialty expertise. The mean outcome prediction from group of providers ("the wisdom of the crowd") may be superior to that of individual providers.
Keywords: Brain injury; Neurological emergencies; Neuroprognostication; Outcome prediction.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Rost NS, Smith EE, Chang Y, Snider RW, Chanderraj R, Schwab K, et al. Prediction of functional outcome in patients with primary intracerebral hemorrhage: The FUNC score. Stroke. 2008;39(8):2304–9. - PubMed
-
- Hemphill JC, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH Score. Stroke. 2001;32(4):891–7. - PubMed
-
- Saposnik G, Kapral MK, Liu Y, Hall R, O’Donnell M, Raptis S, et al. IScore: A risk score to predict death early after hospitalization for an acute ischemic stroke. Circulation. 2011;123(7):739–49. - PubMed
-
- Quinn T, Moskowitz J, Khan MW, Shutter L, Goldberg R, Col N, et al. What Families Need and Physicians Deliver - Contrasting Communication Preferences between Surrogate Decision- Makers and Physicians during Outcome Prognostication in Critically-Ill TBI Patients. Neurocritical. 2017;27(2):154–62. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
