

IL-10 Rescues CLL Survival through Repolarization of Inflammatory Nurse-like Cells
- PMID: 35008174
- PMCID: PMC8750769
- DOI: 10.3390/cancers14010016
IL-10 Rescues CLL Survival through Repolarization of Inflammatory Nurse-like Cells
Abstract
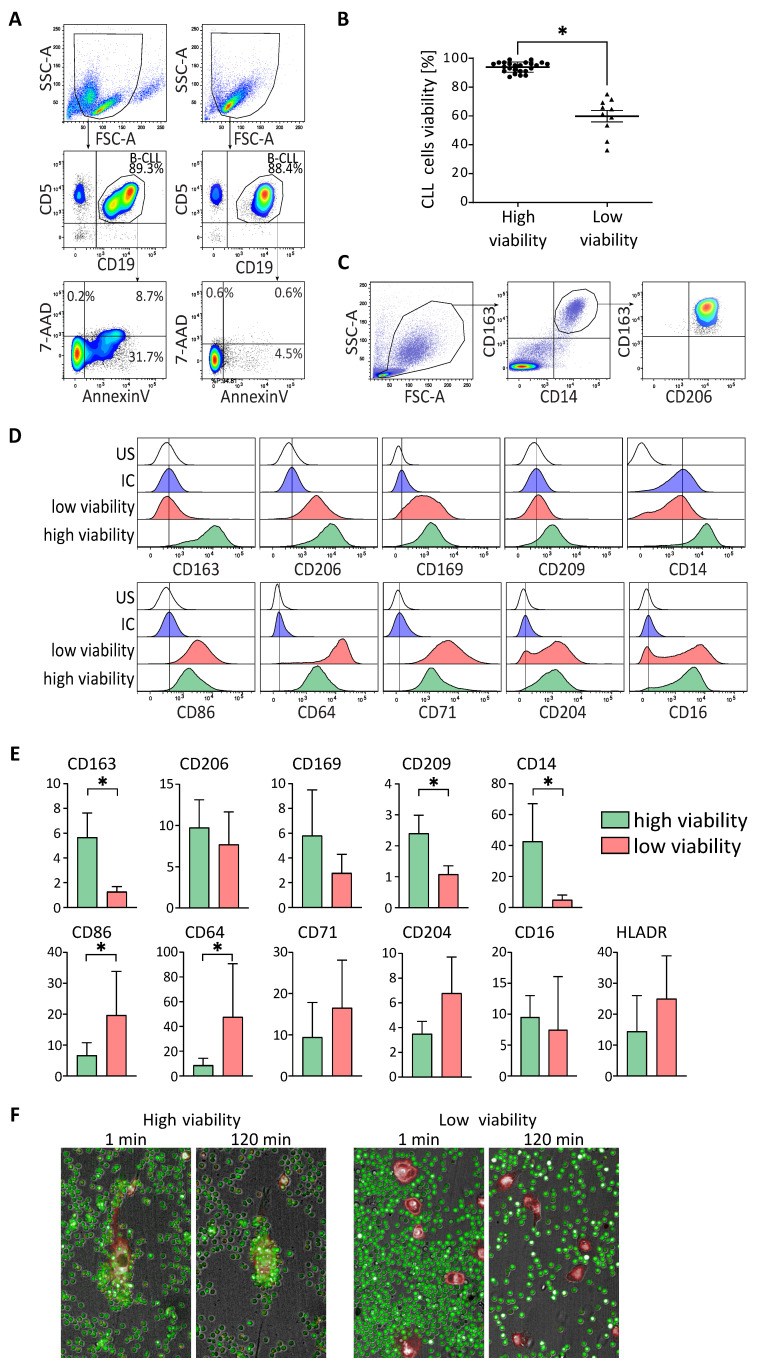
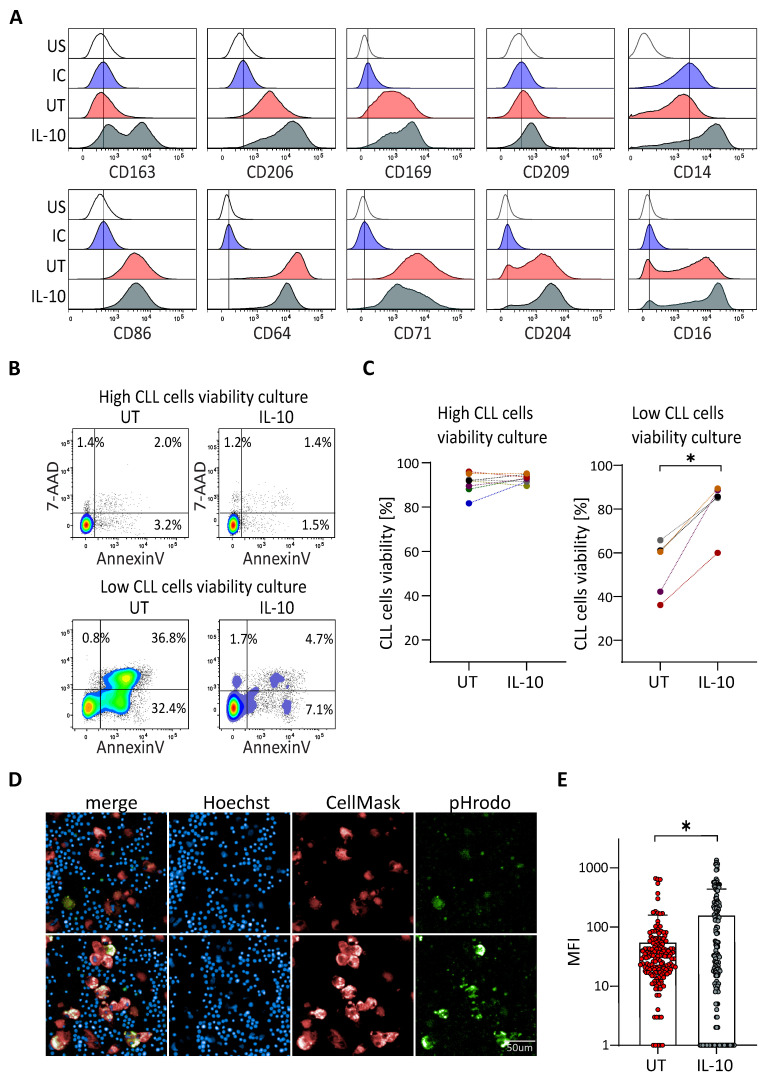
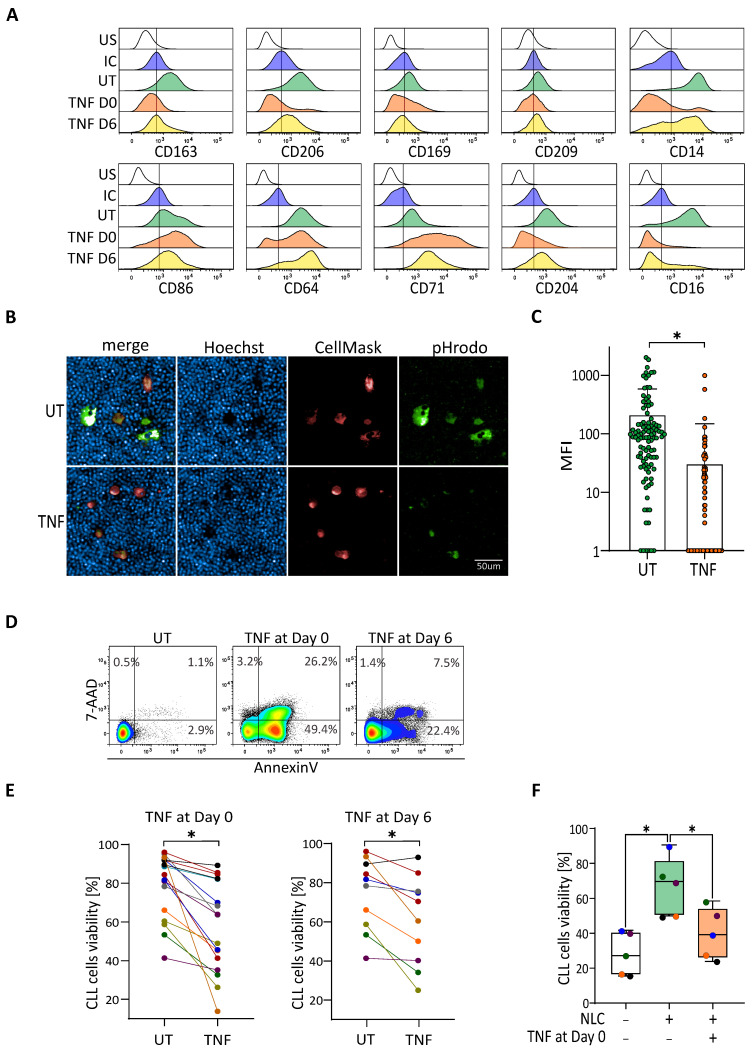
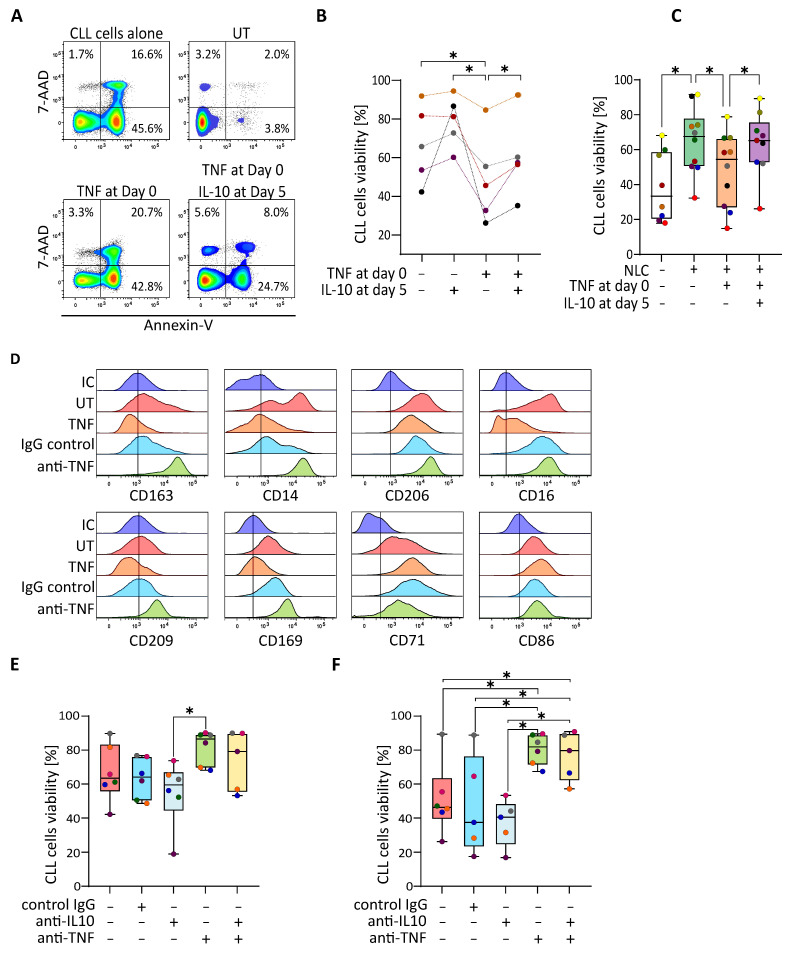
Tumor-associated macrophages (TAMs) in chronic lymphocytic leukemia (CLL) are also called nurse-like cells (NLC), and confer survival signals through the release of soluble factors and cellular contacts. While in most patient samples the presence of NLC in co-cultures guarantees high viability of leukemic cells in vitro, in some cases this protective effect is absent. These macrophages are characterized by an "M1-like phenotype". We show here that their reprogramming towards an M2-like phenotype (tumor-supportive) with IL-10 leads to an increase in leukemic cell survival. Inflammatory cytokines, such as TNF, are also able to depolarize M2-type protective NLC (decreasing CLL cell viability), an effect which is countered by IL-10 or blocking antibodies. Interestingly, both IL-10 and TNF are implied in the pathophysiology of CLL and their elevated level is associated with bad prognosis. We propose that the molecular balance between these two cytokines in CLL niches plays an important role in the maintenance of the protective phenotype of NLCs, and therefore in the survival of CLL cells.
Keywords: CLL; IL-10; Nurse-like cells; TNF; polarization; survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Macrophage Polarization in Chronic Lymphocytic Leukemia: Nurse-Like Cells Are the Caretakers of Leukemic Cells.Biomedicines. 2020 Nov 19;8(11):516. doi: 10.3390/biomedicines8110516. Biomedicines. 2020. PMID: 33228048 Free PMC article. Review.
-
Development of a cell-line model to mimic the pro-survival effect of nurse-like cells in chronic lymphocytic leukemia.Leuk Lymphoma. 2021 Jan;62(1):45-57. doi: 10.1080/10428194.2020.1811274. Epub 2020 Aug 28. Leuk Lymphoma. 2021. PMID: 32856983
-
Circulating microenvironment of CLL: are nurse-like cells related to tumor-associated macrophages?Blood Cells Mol Dis. 2013 Apr;50(4):263-70. doi: 10.1016/j.bcmd.2012.12.003. Epub 2013 Jan 11. Blood Cells Mol Dis. 2013. PMID: 23313631
-
BDNF belongs to the nurse-like cell secretome and supports survival of B chronic lymphocytic leukemia cells.Sci Rep. 2020 Jul 28;10(1):12572. doi: 10.1038/s41598-020-69307-1. Sci Rep. 2020. PMID: 32724091 Free PMC article.
-
Survival and Immunosuppression Induced by Hepatocyte Growth Factor in Chronic Lymphocytic Leukemia.Curr Mol Med. 2017;17(1):24-33. doi: 10.2174/1566524017666170220095838. Curr Mol Med. 2017. PMID: 28231754 Review.
Cited by
-
Nurselike cells sequester B cells in disorganized lymph nodes in chronic lymphocytic leukemia via alternative production of CCL21.Blood Adv. 2022 Aug 23;6(16):4691-4704. doi: 10.1182/bloodadvances.2021006169. Blood Adv. 2022. PMID: 35679464 Free PMC article.
-
Treatment Refractoriness in Chronic Lymphocytic Leukemia: Old and New Molecular Biomarkers.Int J Mol Sci. 2023 Jun 20;24(12):10374. doi: 10.3390/ijms241210374. Int J Mol Sci. 2023. PMID: 37373521 Free PMC article. Review.
-
Macrophage-Based Therapeutic Strategies in Hematologic Malignancies.Cancers (Basel). 2023 Jul 22;15(14):3722. doi: 10.3390/cancers15143722. Cancers (Basel). 2023. PMID: 37509382 Free PMC article. Review.
-
An agent-based model of monocyte differentiation into tumour-associated macrophages in chronic lymphocytic leukemia.iScience. 2023 May 19;26(6):106897. doi: 10.1016/j.isci.2023.106897. eCollection 2023 Jun 16. iScience. 2023. PMID: 37332613 Free PMC article.
-
Analysis of causes for poor persistence of CAR-T cell therapy in vivo.Front Immunol. 2023 Jan 25;14:1063454. doi: 10.3389/fimmu.2023.1063454. eCollection 2023. Front Immunol. 2023. PMID: 36761742 Free PMC article. Review.
References
-
- Caligaris-Cappio F., Gottardi D., Alfarano A., Stacchini A., Gregoretti M.G., Ghia P., Bertero M.T., Novarino A., Bergui L. The nature of the b lymphocyte in b-chronic lymphocytic leukemia. Blood Cells. 1993;19:601–613. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
