

Validation of Breast Cancer Risk Models by Race/Ethnicity, Family History and Molecular Subtypes
- PMID: 35008209
- PMCID: PMC8750569
- DOI: 10.3390/cancers14010045
Validation of Breast Cancer Risk Models by Race/Ethnicity, Family History and Molecular Subtypes
Abstract
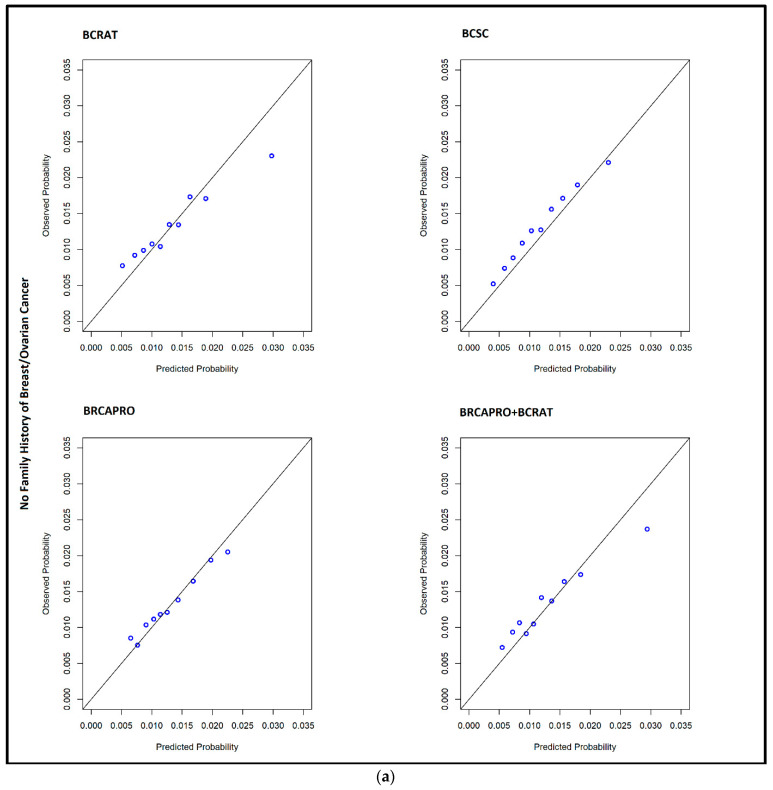
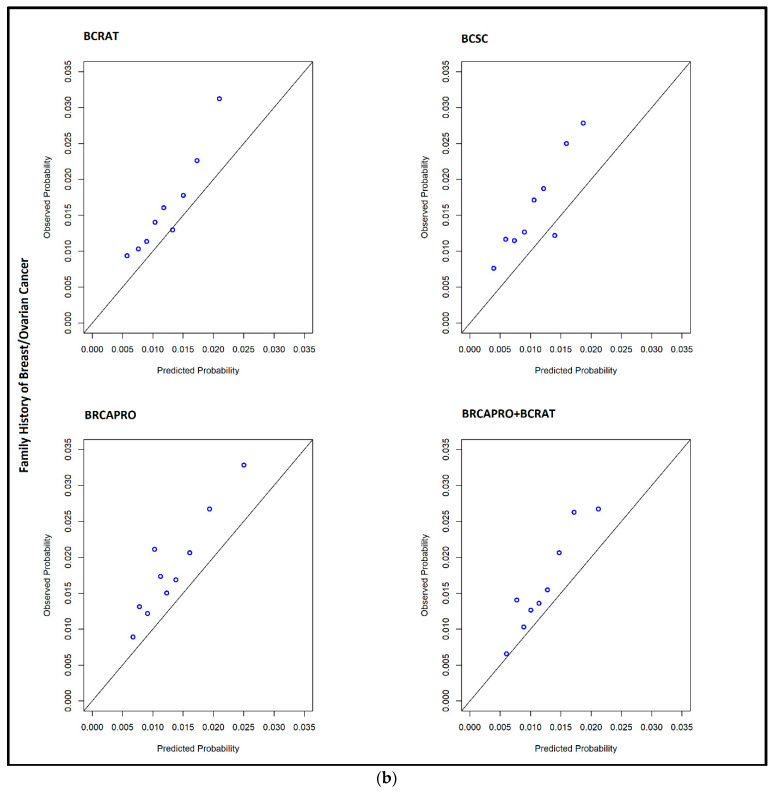
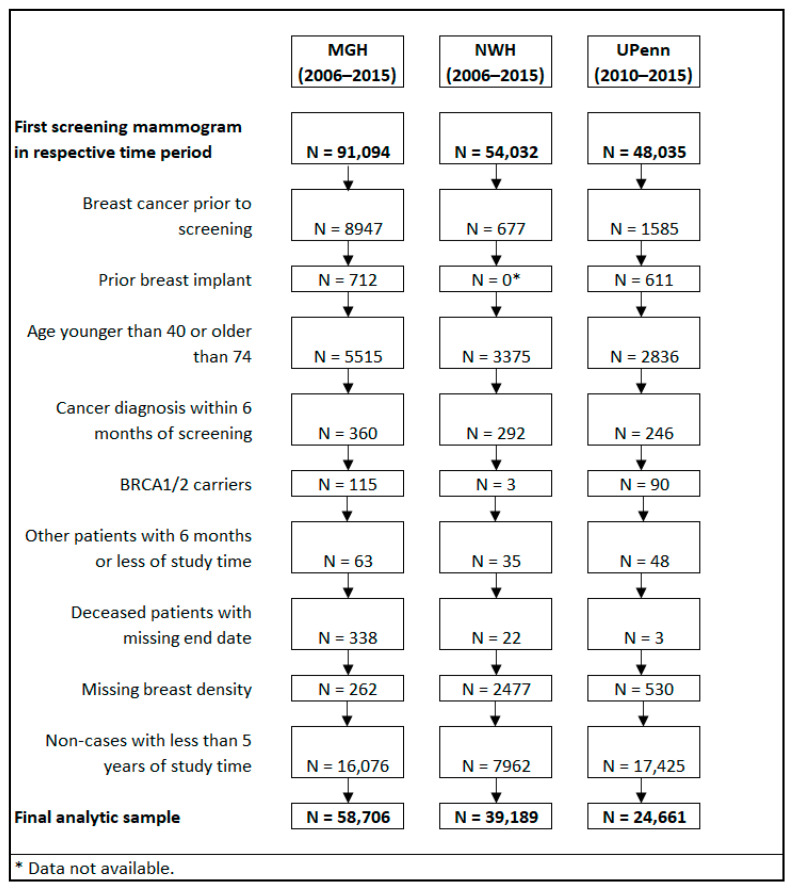
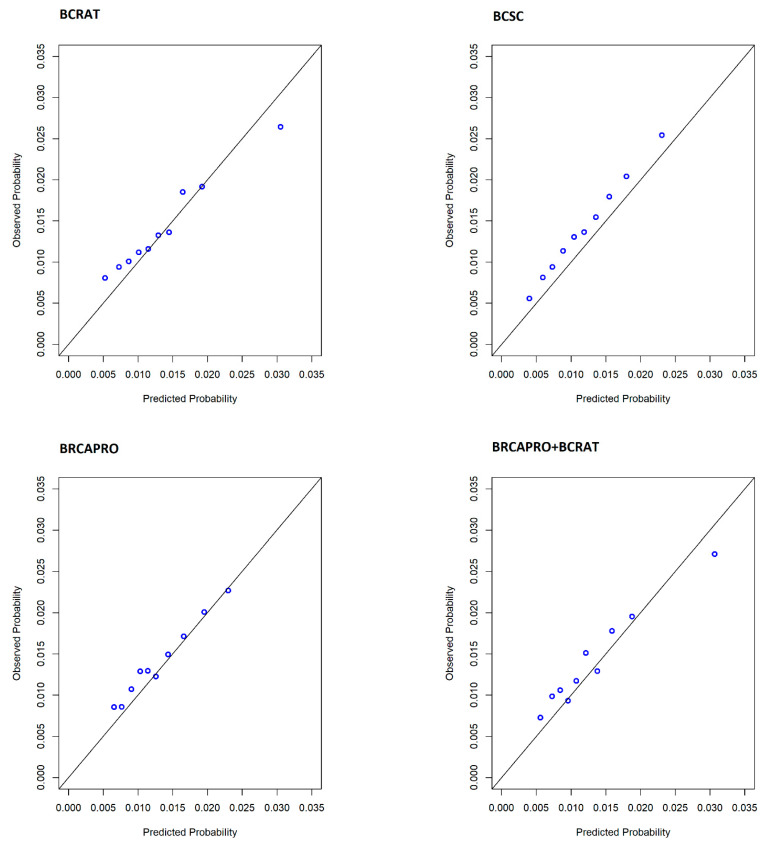
(1) Background: The purpose of this study is to compare the performance of four breast cancer risk prediction models by race, molecular subtype, family history of breast cancer, age, and BMI. (2) Methods: Using a cohort of women aged 40-84 without prior history of breast cancer who underwent screening mammography from 2006 to 2015, we generated breast cancer risk estimates using the Breast Cancer Risk Assessment tool (BCRAT), BRCAPRO, Breast Cancer Surveillance Consortium (BCSC) and combined BRCAPRO+BCRAT models. Model calibration and discrimination were compared using observed-to-expected ratios (O/E) and the area under the receiver operator curve (AUC) among patients with at least five years of follow-up. (3) Results: We observed comparable discrimination and calibration across models. There was no significant difference in model performance between Black and White women. Model discrimination was poorer for HER2+ and triple-negative subtypes compared with ER/PR+HER2-. The BRCAPRO+BCRAT model displayed improved calibration and discrimination compared to BRCAPRO among women with a family history of breast cancer. Across models, discriminatory accuracy was greater among obese than non-obese women. When defining high risk as a 5-year risk of 1.67% or greater, models demonstrated discordance in 2.9% to 19.7% of patients. (4) Conclusions: Our results can inform the implementation of risk assessment and risk-based screening among women undergoing screening mammography.
Keywords: breast cancer; mammography; risk prediction.
Conflict of interest statement
Giovanni Parmigiani is a co-founder and equity holder in Phaeno Biotechnologies, a member of the Scientific Advisory Board of Konica-Minolta Precision Medicine (which includes Ambry Genetics and Invicro), and a consultant for Delfi Diagnostics and Foundation Medicine. Danielle Braun and Giovanni Parmigiani co-lead the BayesMendel lab, which develops and maintains the BayesMendel software package. This includes a variety of risk assessment tools including BRCAPRO, PancPRO, MelaPRO, MMRpro, and PanelPRO and is licensed for commercial use. All licensing revenues are used for software maintenance and upgrades. Neither BayesMendel lab leaders nor members derive personal income from BayesMendel licenses. Danielle Braun and Giovanni Parmigiani are co-inventor of the Ask2me tool, which is commercially licensed. Kevin Hughes receives honoraria from Hologic (surgical implant for radiation planning with breast conservation and wire free breast biopsy) and Myriad Genetics, Hughes has financial interests in CRA Health (Formerly Hughes RiskApps) which recently was sold to Volpara. CRA Health develops risk assessment models/software with a particular focus on breast cancer and colorectal cancer. Hughes is a founder of the company. Hughes is the Co-Creator of Ask2Me.Org which is freely available for clinical use and is licensed for commercial use by the Dana Farber Cancer Institute and the MGH. Hughes’s interests in CRA Health and Ask2Me.Org were reviewed and are managed by Massachusetts General Hospital and Partners Health Care in accordance with their conflict-of-interest policies. Constance Lehman is co-founder of Clairity, which is developing an AI-based risk assessment products. Lehman’s interests in Clairity were reviewed and are managed by Massachusetts General Hospital and Partners Health Care in accordance with their conflict-of-interest policies. Emily Conant is on the grant and advisory boards for iCAD, Inc. and Hologic, Inc. The remaining authors have no conflicts to disclose. The funders of this study had no role in its design; the collection, analyses, or interpretation of the data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Does the Presence of Missing Data Affect the Performance of the SORG Machine-learning Algorithm for Patients With Spinal Metastasis? Development of an Internet Application Algorithm.Clin Orthop Relat Res. 2024 Jan 1;482(1):143-157. doi: 10.1097/CORR.0000000000002706. Epub 2023 Jun 12. Clin Orthop Relat Res. 2024. PMID: 37306629 Free PMC article.
-
Feasibility of risk assessment for breast cancer molecular subtypes.Breast Cancer Res Treat. 2024 Nov;208(1):103-110. doi: 10.1007/s10549-024-07404-9. Epub 2024 Jun 25. Breast Cancer Res Treat. 2024. PMID: 38916820 Free PMC article.
-
Mammography in combination with breast ultrasonography versus mammography for breast cancer screening in women at average risk.Cochrane Database Syst Rev. 2023 Mar 31;3(3):CD009632. doi: 10.1002/14651858.CD009632.pub3. Cochrane Database Syst Rev. 2023. PMID: 36999589 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
Cited by
-
Variability Among Breast Cancer Risk Classification Models When Applied at the Level of the Individual Woman.J Gen Intern Med. 2023 Aug;38(11):2584-2592. doi: 10.1007/s11606-023-08043-4. Epub 2023 Feb 7. J Gen Intern Med. 2023. PMID: 36749434 Free PMC article.
-
Impact of Affordable Care Act Provisions on the Racial Makeup of Patients Enrolled at a Deep South, High-Risk Breast Cancer Clinic.J Racial Ethn Health Disparities. 2024 Sep 5:10.1007/s40615-024-02104-y. doi: 10.1007/s40615-024-02104-y. Online ahead of print. J Racial Ethn Health Disparities. 2024. PMID: 39235712
-
A nomogram for predicting overall survival of breast cancer with regional lymph node metastasis in young women.Transl Cancer Res. 2024 Feb 29;13(2):542-557. doi: 10.21037/tcr-23-1825. Epub 2024 Feb 22. Transl Cancer Res. 2024. PMID: 38482426 Free PMC article.
-
External Validation of a Mammography-Derived AI-Based Risk Model in a U.S. Breast Cancer Screening Cohort of White and Black Women.Cancers (Basel). 2022 Sep 30;14(19):4803. doi: 10.3390/cancers14194803. Cancers (Basel). 2022. PMID: 36230723 Free PMC article.
-
Inequities in referrals to a breast cancer risk assessment and prevention clinic: a mixed methods study.BMC Prim Care. 2023 Aug 25;24(1):165. doi: 10.1186/s12875-023-02126-1. BMC Prim Care. 2023. PMID: 37626335 Free PMC article.
References
-
- Cintolo-Gonzalez J.A., Braun D., Blackford A.L., Mazzola E., Acar A., Plichta J.K., Griffin M., Hughes K.S. Breast cancer risk models: A comprehensive overview of existing models, validation, and clinical applications. Breast Cancer Res. Treat. 2017;164:263–284. doi: 10.1007/s10549-017-4247-z. - DOI - PubMed
-
- Banegas M.P., John E.M., Slattery M.L., Gomez S.L., Yu M., LaCroix A.Z., Pee D., Chlebowski R.T., Hines L.M., Thompson C.A., et al. Projecting Individualized Absolute Invasive Breast Cancer Risk in US Hispanic Women. J. Natl. Cancer Inst. 2017;109:djw215. doi: 10.1093/jnci/djw215. - DOI - PMC - PubMed
-
- Gail M.H., Costantino J.P., Pee D., Bondy M., Newman L., Selvan M., Anderson G.L., Malone K.E., Marchbanks P.A., McCaskill-Stevens W., et al. Projecting individualized absolute invasive breast cancer risk in African American women. J. Natl. Cancer Inst. 2007;99:1782–1792. doi: 10.1093/jnci/djm223. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
