

Adenoma to Colorectal Cancer Estimated Transition Rates Stratified by BMI Categories-A Cross-Sectional Analysis of Asymptomatic Individuals from Screening Colonoscopy Program
- PMID: 35008224
- PMCID: PMC8750540
- DOI: 10.3390/cancers14010062
Adenoma to Colorectal Cancer Estimated Transition Rates Stratified by BMI Categories-A Cross-Sectional Analysis of Asymptomatic Individuals from Screening Colonoscopy Program
Abstract
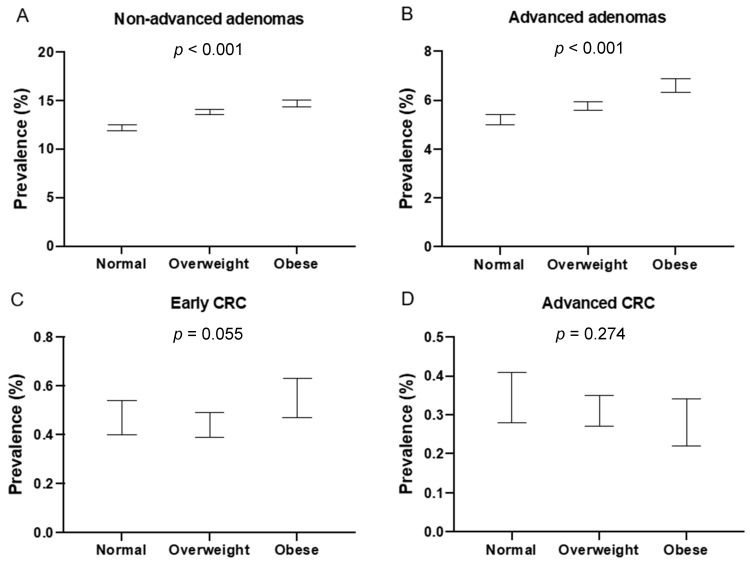
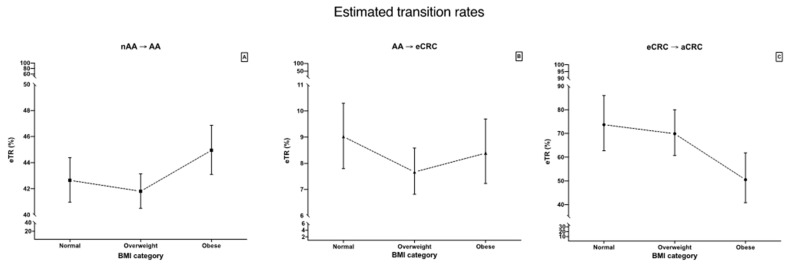
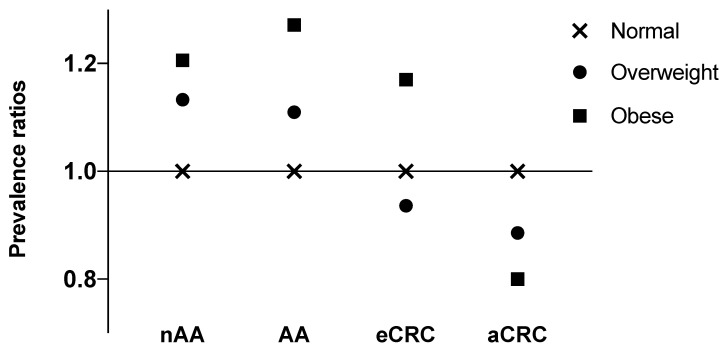
Most colorectal cancers (CRC) assumedly develop from precursor lesions, i.e., colorectal adenomas (adenoma-carcinoma sequence). Epidemiological and clinical data supporting this hypothesis are limited. Therefore, the aim of the present study is to estimate relative dynamics of colorectal adenoma-carcinoma sequence for groups of screenees stratified by BMI (body mass index) based on prevalence data from Polish Colonoscopy Screening Program (PCSP). We performed a cross-sectional analysis of database records of individuals who entered the national opportunistic colonoscopy screening program for CRC in Poland. We calculated prevalence of adenomas and CRCs adjusted for sex, 5-year age group, family history of CRC, smoking, diabetes and use of aspirin, hormonal therapy and proton-pump inhibitors use. Thereafter we calculated estimated transition rate (eTR) with confidence intervals (CIs) defined as adjusted prevalence of more advanced lesion divided by adjusted prevalence of less advanced lesion. All analyzes were stratified according to the BMI categories: normal (BMI 18.0 to <25.0), overweight (BMI 25.0 to <30.0) and obese (BMI ≥ 30.0). Results are reported in the same respective order. After exclusions we performed analyses on 147,385 individuals. We found that prevalence of non-advanced adenomas is increasing with BMI category (12.19%, 13.81%, 14.70%, respectively; p < 0.001). Prevalence of advanced adenomas was increasing with BMI category (5.20%, 5.77%, 6.61%, respectively; p < 0.001). Early CRCs prevalence was the highest for obese individuals (0.55%) and the lowest for overweight individuals (0.44%) with borderline significance (p = 0.055). For advanced CRC we found that prevalence seems to be inversely related to BMI category, however no statistically significant differences were observed (0.35%, 0.31%, 0.28%; p = 0.274). eTR for non-advanced adenoma to advanced adenoma is higher for obese individuals than for overweight individuals with bordering CIs (42.65% vs. 41.81% vs. 44.95%) eTR for advanced adenoma to early CRC is highest for normal individuals, however CIs are overlapping with remaining BMI categories (9.02% vs. 7.67% vs. 8.39%). eTR for early CRC to advanced CRC is lower for obese individuals in comparison to both normal and overweight individuals with marginally overlapping CIs (73.73% vs. 69.90% vs. 50.54%). Obese individuals are more likely to develop adenomas, advanced adenomas and early CRC but less likely to progress to advanced CRC. Therefore, this study provides new evidence that obesity paradox exists for colorectal cancer.
Keywords: colonoscopy; colorectal adenoma; colorectal cancer; colorectal cancer epidemiology; colorectal cancer prevalence; screening.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Clinical stages of colorectal cancer diagnosed in obese and overweight individuals in the Polish Colonoscopy Screening Program.United European Gastroenterol J. 2019 Jul;7(6):790-797. doi: 10.1177/2050640619840451. Epub 2019 Mar 21. United European Gastroenterol J. 2019. PMID: 31316783 Free PMC article.
-
Adenoma, advanced adenoma and colorectal cancer prevalence in asymptomatic 40- to 49-year-old subjects with a first-degree family history of colorectal cancer.Colorectal Dis. 2013 Sep;15(9):1093-9. doi: 10.1111/codi.12263. Colorectal Dis. 2013. PMID: 23627814
-
Association of Adenoma Detection Rate and Adenoma Characteristics With Colorectal Cancer Mortality After Screening Colonoscopy.Clin Gastroenterol Hepatol. 2021 Sep;19(9):1890-1898. doi: 10.1016/j.cgh.2021.04.023. Epub 2021 Apr 18. Clin Gastroenterol Hepatol. 2021. PMID: 33878471
-
Global Prevalence of Colorectal Neoplasia: A Systematic Review and Meta-Analysis.Clin Gastroenterol Hepatol. 2020 Mar;18(3):553-561.e10. doi: 10.1016/j.cgh.2019.07.016. Epub 2019 Jul 16. Clin Gastroenterol Hepatol. 2020. PMID: 31323383
-
High-risk family colorectal cancer screening service in Ireland: Critical review of clinical outcomes.Cancer Epidemiol. 2017 Oct;50(Pt A):30-38. doi: 10.1016/j.canep.2017.07.002. Epub 2017 Aug 4. Cancer Epidemiol. 2017. PMID: 28783501 Review.
Cited by
-
The Protective Effect of Bariatric Surgery on the Development of Colorectal Cancer: A Systematic Review and Meta-Analysis.Int J Environ Res Public Health. 2023 Feb 23;20(5):3981. doi: 10.3390/ijerph20053981. Int J Environ Res Public Health. 2023. PMID: 36900989 Free PMC article.
-
Screening for liver fibrosis: lessons from colorectal and lung cancer screening.Nat Rev Gastroenterol Hepatol. 2024 Jul;21(7):517-527. doi: 10.1038/s41575-024-00907-2. Epub 2024 Mar 13. Nat Rev Gastroenterol Hepatol. 2024. PMID: 38480849 Review.
-
Current Perspectives on Colorectal Cancer Screening and Surveillance in the Geriatric Population.Curr Gastroenterol Rep. 2025 Jun 2;27(1):34. doi: 10.1007/s11894-025-00985-5. Curr Gastroenterol Rep. 2025. PMID: 40455318 Review.
References
-
- AJCC AJCC Colorectal Cancer Stages. [(accessed on 9 January 2019)]. Available online: https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-st....
LinkOut - more resources
Full Text Sources
