

Diagnosis of Glioblastoma by Immuno-Positron Emission Tomography
- PMID: 35008238
- PMCID: PMC8750680
- DOI: 10.3390/cancers14010074
Diagnosis of Glioblastoma by Immuno-Positron Emission Tomography
Abstract
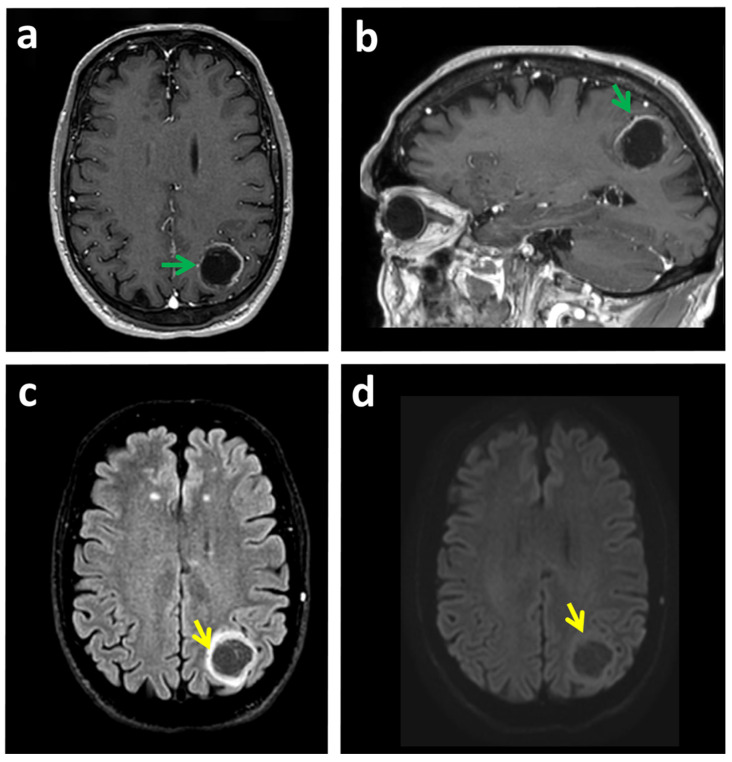
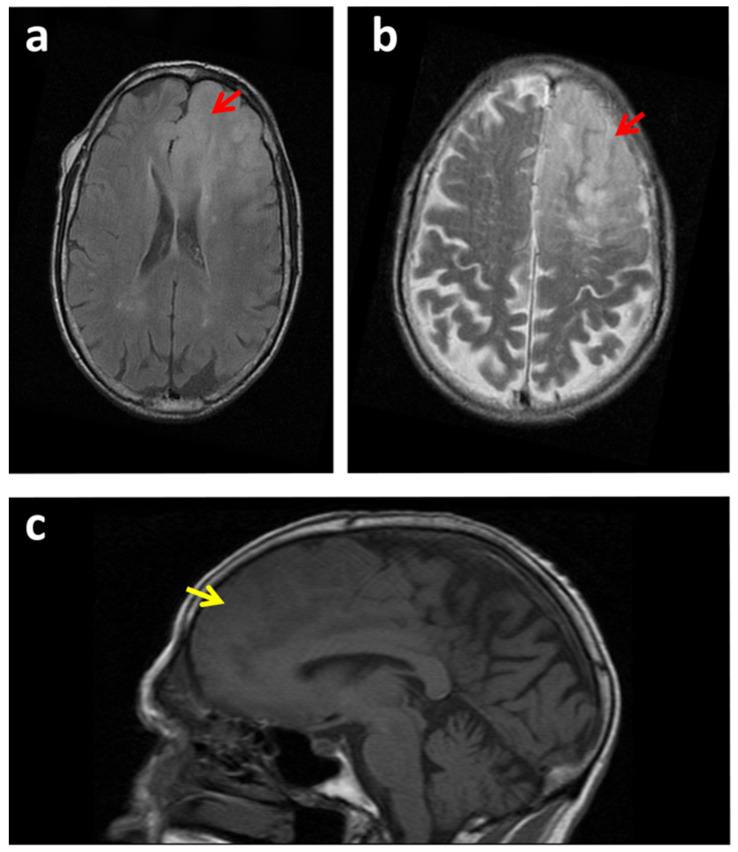
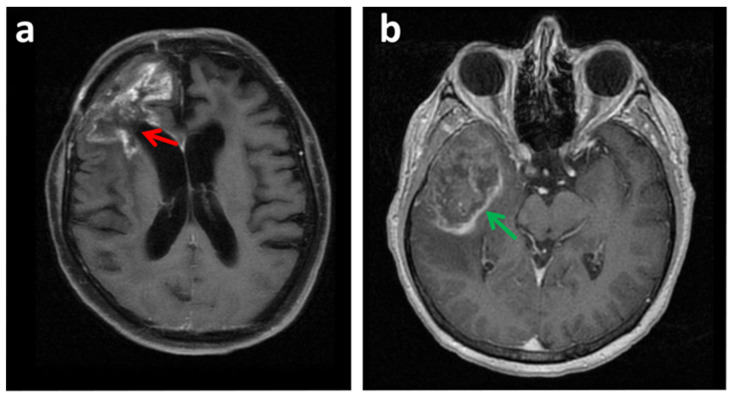
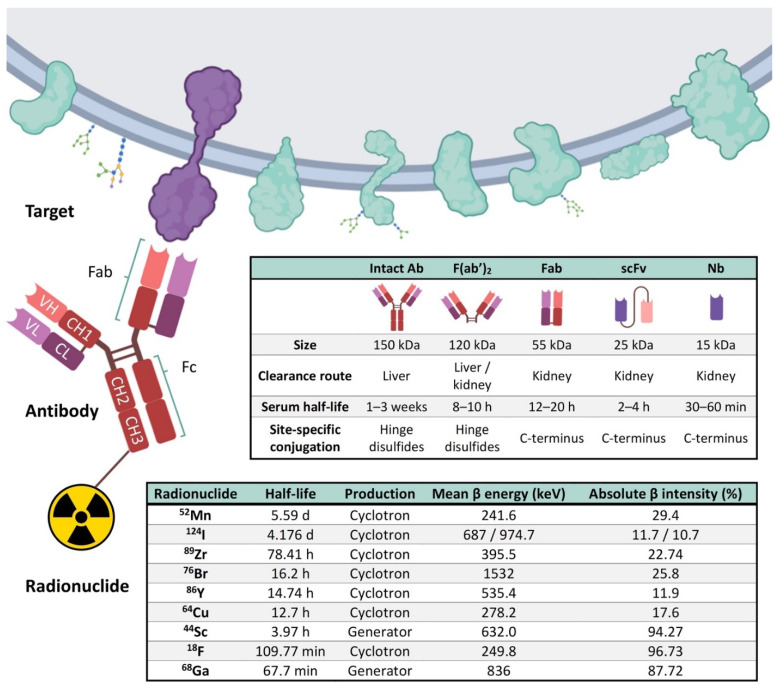
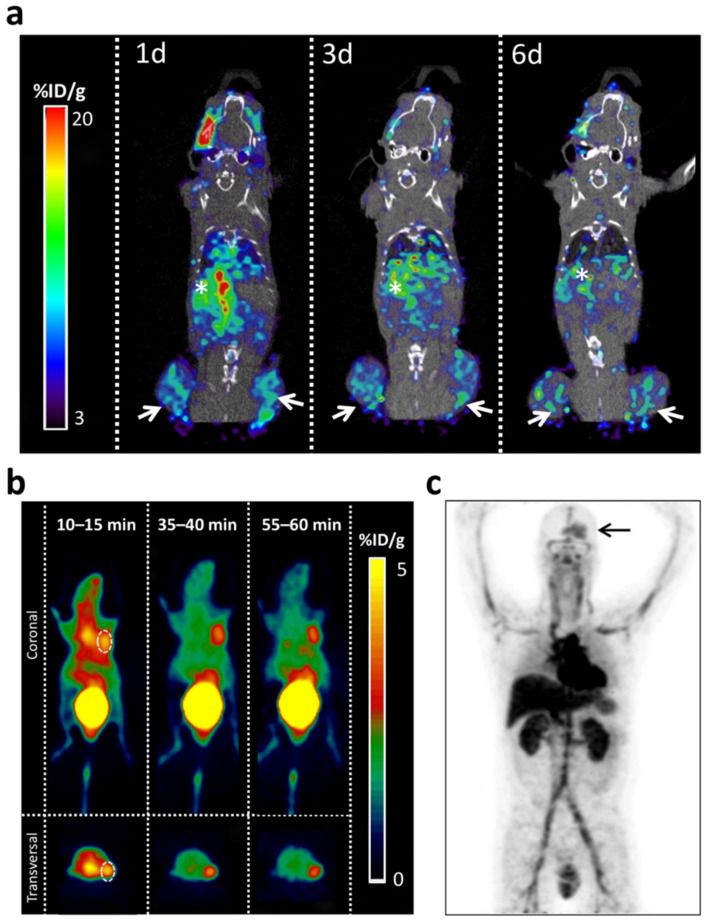
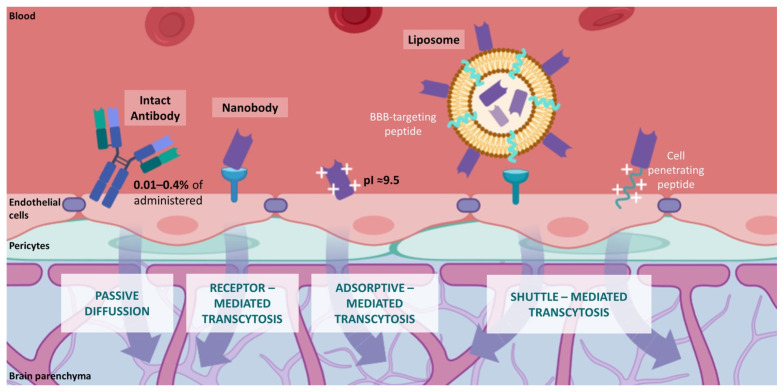
Neuroimaging has transformed neuro-oncology and the way that glioblastoma is diagnosed and treated. Magnetic Resonance Imaging (MRI) is the most widely used non-invasive technique in the primary diagnosis of glioblastoma. Although MRI provides very powerful anatomical information, it has proven to be of limited value for diagnosing glioblastomas in some situations. The final diagnosis requires a brain biopsy that may not depict the high intratumoral heterogeneity present in this tumor type. The revolution in "cancer-omics" is transforming the molecular classification of gliomas. However, many of the clinically relevant alterations revealed by these studies have not yet been integrated into the clinical management of patients, in part due to the lack of non-invasive biomarker-based imaging tools. An innovative option for biomarker identification in vivo is termed "immunotargeted imaging". By merging the high target specificity of antibodies with the high spatial resolution, sensitivity, and quantitative capabilities of positron emission tomography (PET), "Immuno-PET" allows us to conduct the non-invasive diagnosis and monitoring of patients over time using antibody-based probes as an in vivo, integrated, quantifiable, 3D, full-body "immunohistochemistry" in patients. This review provides the state of the art of immuno-PET applications and future perspectives on this imaging approach for glioblastoma.
Keywords: antibody; diagnostic imaging; glioblastoma; immuno-PET; molecular imaging; nanobody; neuroimaging; theragnostic probes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Verhaak R.G.W., Hoadley K.A., Purdom E., Wang V., Qi Y., Wilkerson M.D., Miller C.R., Ding L., Golub T., Mesirov J.P., et al. Integrated Genomic Analysis Identifies Clinically Relevant Subtypes of Glioblastoma Characterized by Abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell. 2010;17:98–110. doi: 10.1016/j.ccr.2009.12.020. - DOI - PMC - PubMed
-
- Deb P., Sharma M.C., Mahapatra A.K., Agarwal D., Sarkar C. Glioblastoma multiforme with long term survival. Neurol. India. 2005;53:329–332. - PubMed
Publication types
Grants and funding
- PI18/01665/Instituto de Salud Carlos III
- XIII Beca FERO en Investigación Oncológica Traslacional/Fundación FERO
- I Ayuda a la investigación del cáncer infantil/Asociación de Padres de Niños con Cáncer de Aragón (ASPANOA)
- PRDAR17002RUIZ/Asociación Española Contra el Cáncer
- PRDAR18006MEND/Asociación Española Contra el Cáncer
LinkOut - more resources
Full Text Sources
